

Boosters every 4 months for the Elderly?
Boosters every 4 months for the Elderly?
Post #781

The CDC looks to be finally coming around to reducing their recommendations for COVID shot boosters for the younger ages (catching up with the rest of the world):
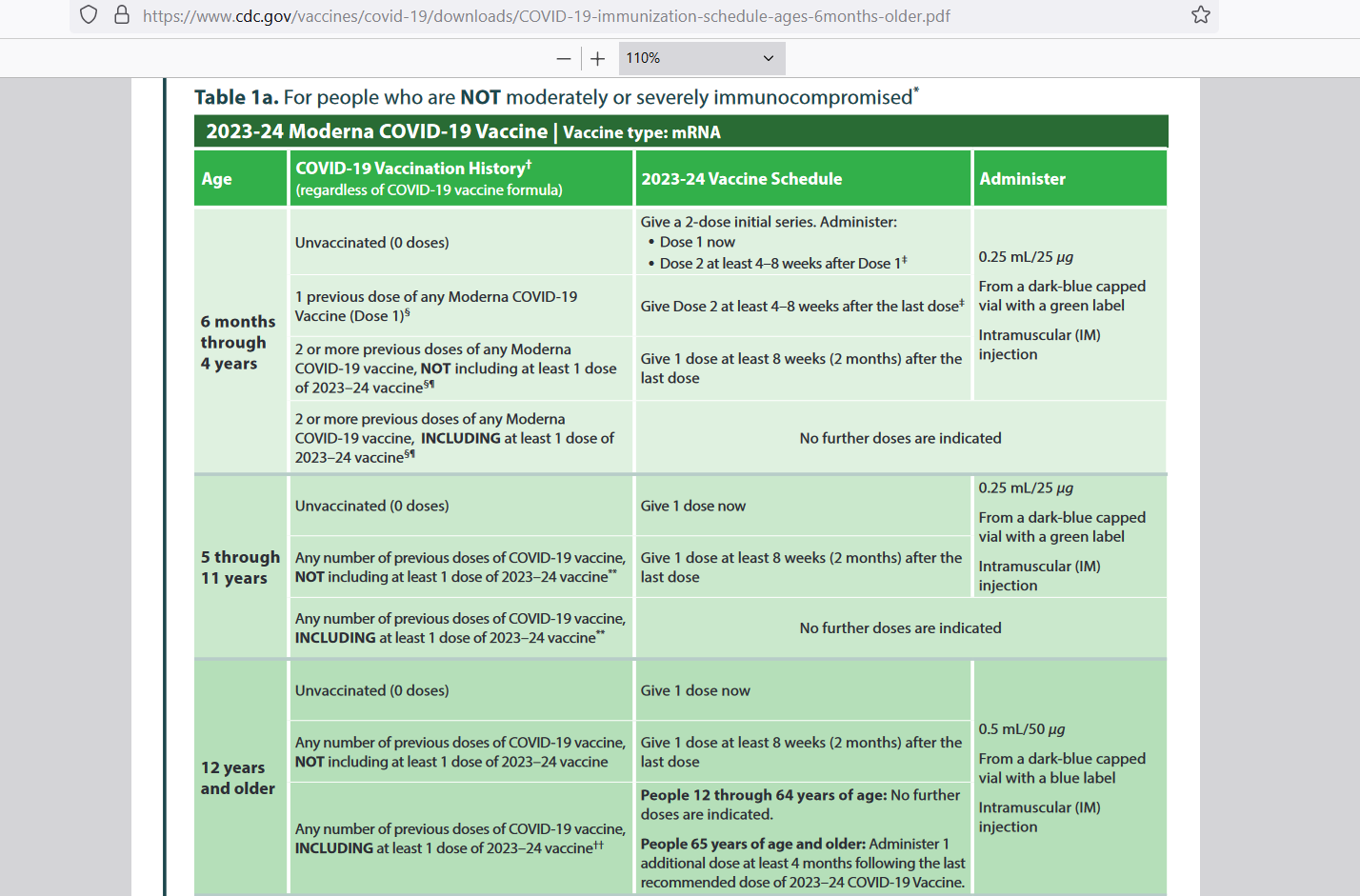
But check out how they tell those over age 64 to get a booster 4 months after the last one. If this schedule were to repeat itself, then elderly would get 3 boosters per year. But when you track the adverse events reported to VAERS for Moderna, and then scale the reports appropriately so as to estimate the true underlying rate, it’s risky.
How Risky?
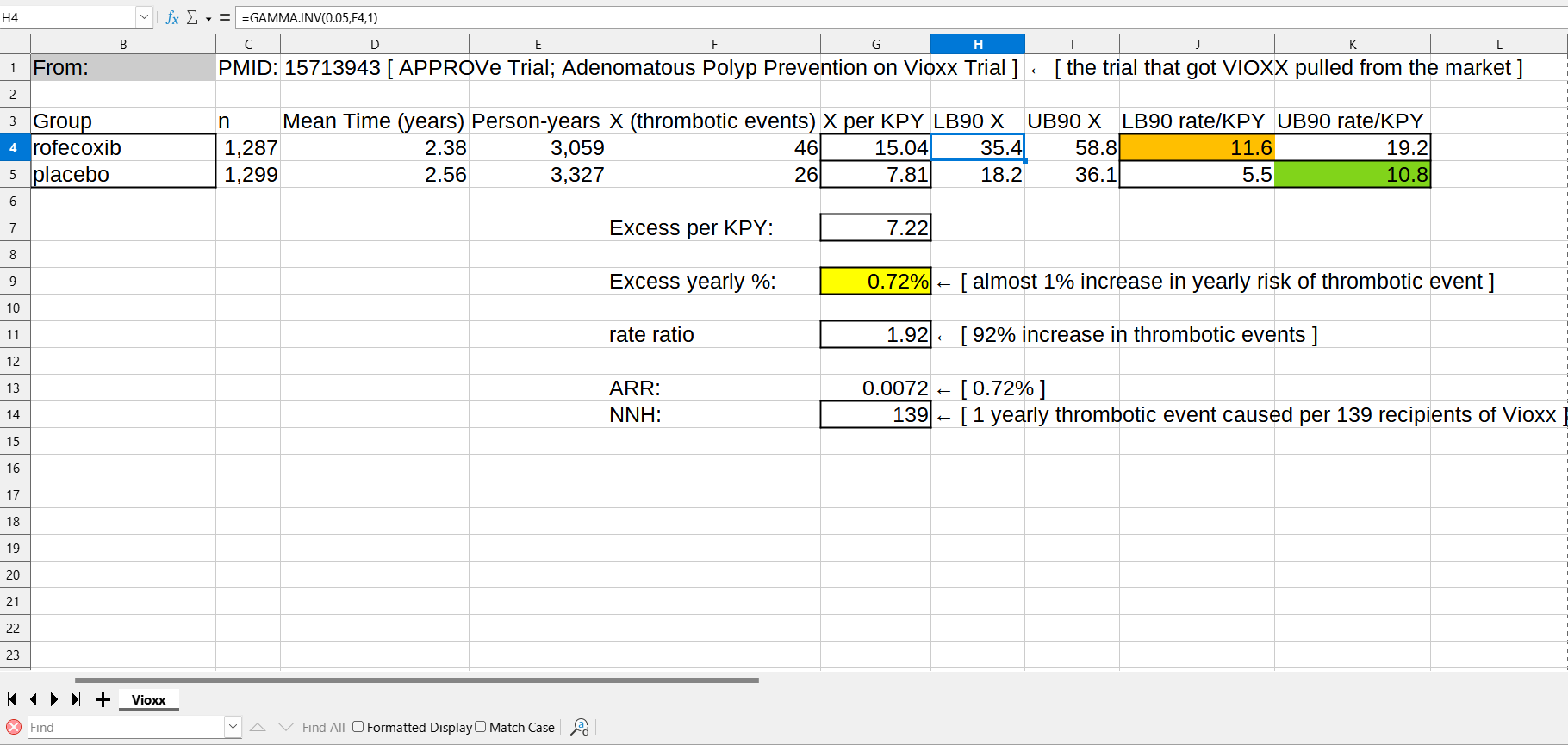
Back in 2004, after 80 million prescriptions for it had been written, Vioxx (rofecoxib) was pulled off of the market due to increased risk of thrombotic events. Vioxx had been wildly successful and was very popular, but the risk proved to be too much to handle. The excess in risk of thrombotic events was 0.7% yearly (yellow cell):
But when the reporting rate for Moderna of serious adverse event reports (serious AERs) — serious means required at least hospitalization — is scaled up to estimate the true rate using the median rate of capture of adverse events of 6% underlying events making it into VAERS, you get a risk of hospitalization higher than Vioxx:

Cell B27 shows 252 million Moderna shots by 22 Mar 2023, and cell E27 shows the number of serious AERs in VAERS by 31 Mar 2023. Cell F33 shows the yearly risk of being put into the hospital due to taking 3 Moderna shots per year: 0.9%, which is higher than the 0.72% which got Vioxx pulled from the market.
Also notice how an extra yearly death is expected for each 500 who are tripled-dosed (2 deaths per 1,000 triple-dosed). But what is insane about this is that the risk of death from COVID is now less than the risk of death from flu. While the Pfizer shots have a somewhat better VAERS reporting rate than Moderna, it is not that much better.
It doesn’t justify a continuation of COVID shots.
Reference
[CDC proposed COVID shot schedule] — https://www.cdc.gov/vaccines/covid-19/downloads/COVID-19-immunization-schedule-ages-6months-older.pdf
[trial that go Vioxx pulled] — Bresalier RS, Sandler RS, Quan H, Bolognese JA, Oxenius B, Horgan K, Lines C, Riddell R, Morton D, Lanas A, Konstam MA, Baron JA; Adenomatous Polyp Prevention on Vioxx (APPROVe) Trial Investigators. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med. 2005 Mar 17;352(11):1092-102. doi: 10.1056/NEJMoa050493. Epub 2005 Feb 15. Erratum in: N Engl J Med. 2006 Jul 13;355(2):221. PMID: 15713943. https://pubmed.ncbi.nlm.nih.gov/15713943/
[median capture rate of passive surveillance is 6% (94% under-reporting rate)] — Hazell L, Shakir SA. Under-reporting of adverse drug reactions : a systematic review. Drug Saf. 2006;29(5):385-96. doi: 10.2165/00002018-200629050-00003. PMID: 16689555. https://pubmed.ncbi.nlm.nih.gov/16689555/
The mass human experiment rolls on, reinforced by the elimination of informed consent.
This is the "new normal;" that we are attending an increasing number of funerals where the cause of death is misrepresented or "unknown."
This is winner take all. Considering how many have already died from the vaccine and how many more are going to die. I declare victory. Already.
So easy was it, that we didn’t have to DO anything.
Just not kill and maim ourselves and one another.
- Like they did.