

Myocarditis 3,700 times more Fatal
Myocarditis 3,700 times more Fatal
Post #904

In those under age 20, there was never any serious risk of dying of COVID:
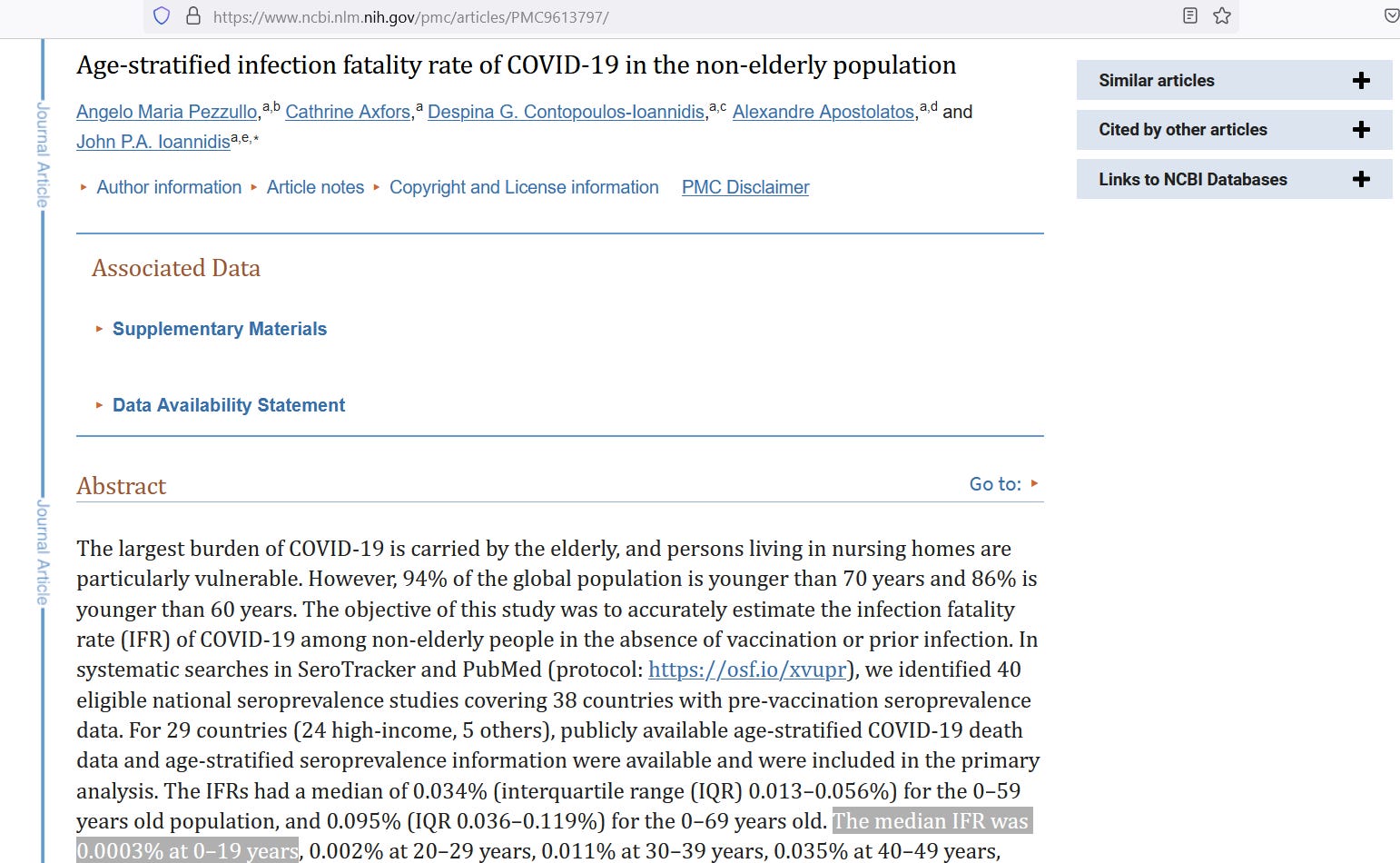
The value at lower left is not even one-thousandth of 1%. But there is a serious risk of dying of myocarditis. For those who are non-elderly (under age 60), the risk of dying of myocarditis is 1.1%:
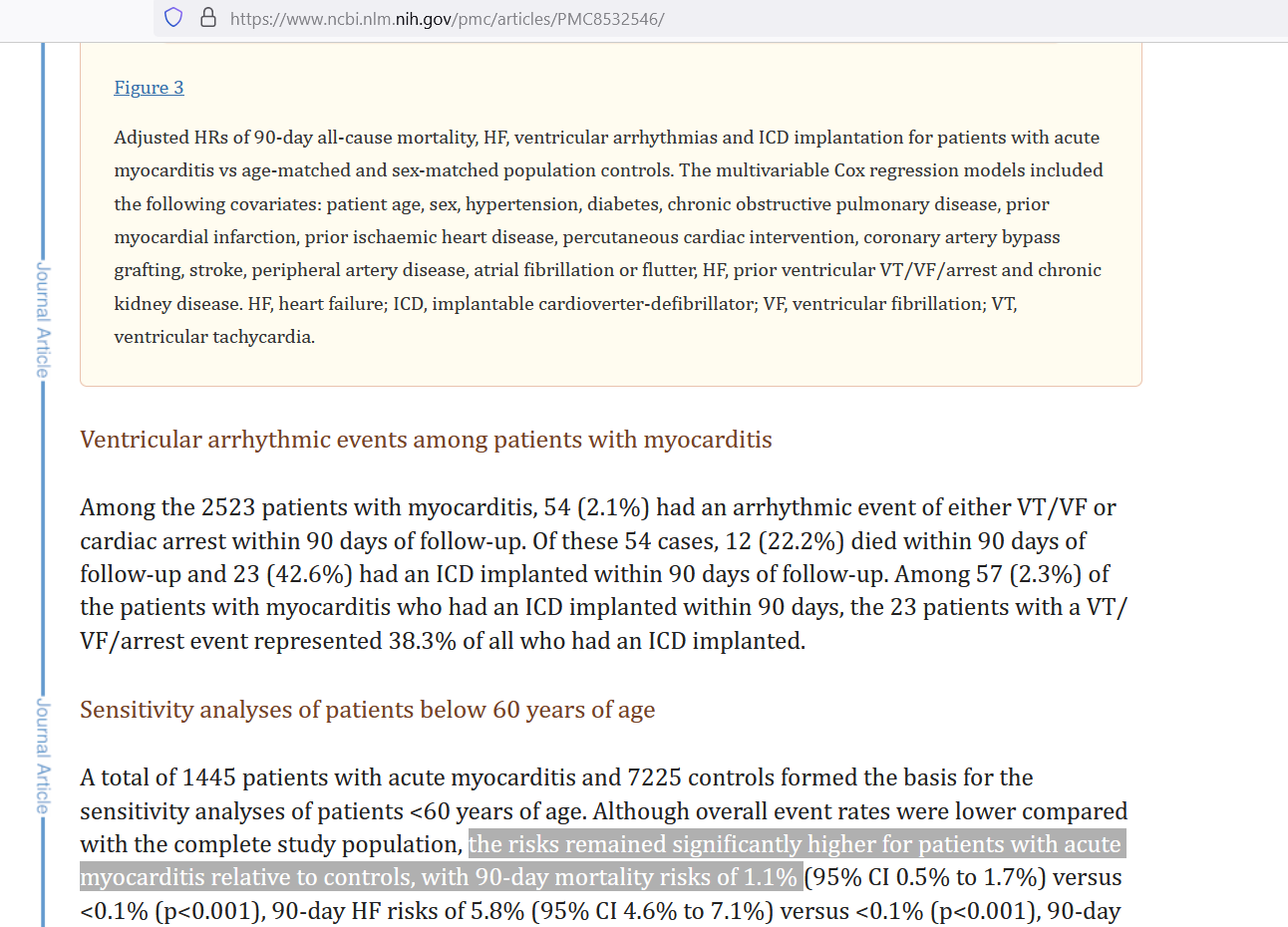
Notice that the age-matched, sex-matched control group died at a rate of <0.1% — meaning that nearly all of the 1.1% risk of death from myocarditis was excess risk, or risk than can be attributed to myocarditis rather than to background factors.
Using half the reporting rate found in young Nordic males (~140 cases per million doses), along with the 672.61 million COVID shot doses up to March 2023, an approximate number of cases of myocarditis caused by COVID shots approaches 50,000 — or approximately 70 myocarditis cases per million COVID shot doses.
Hong Kong data are much higher than this, but we’ll first ignore that.
If all 50,000 myocarditis cases were somehow funneled into those of age 20-29, here is a side-by-side comparison of the expected death count versus what is expected from 50,000 cases of COVID:
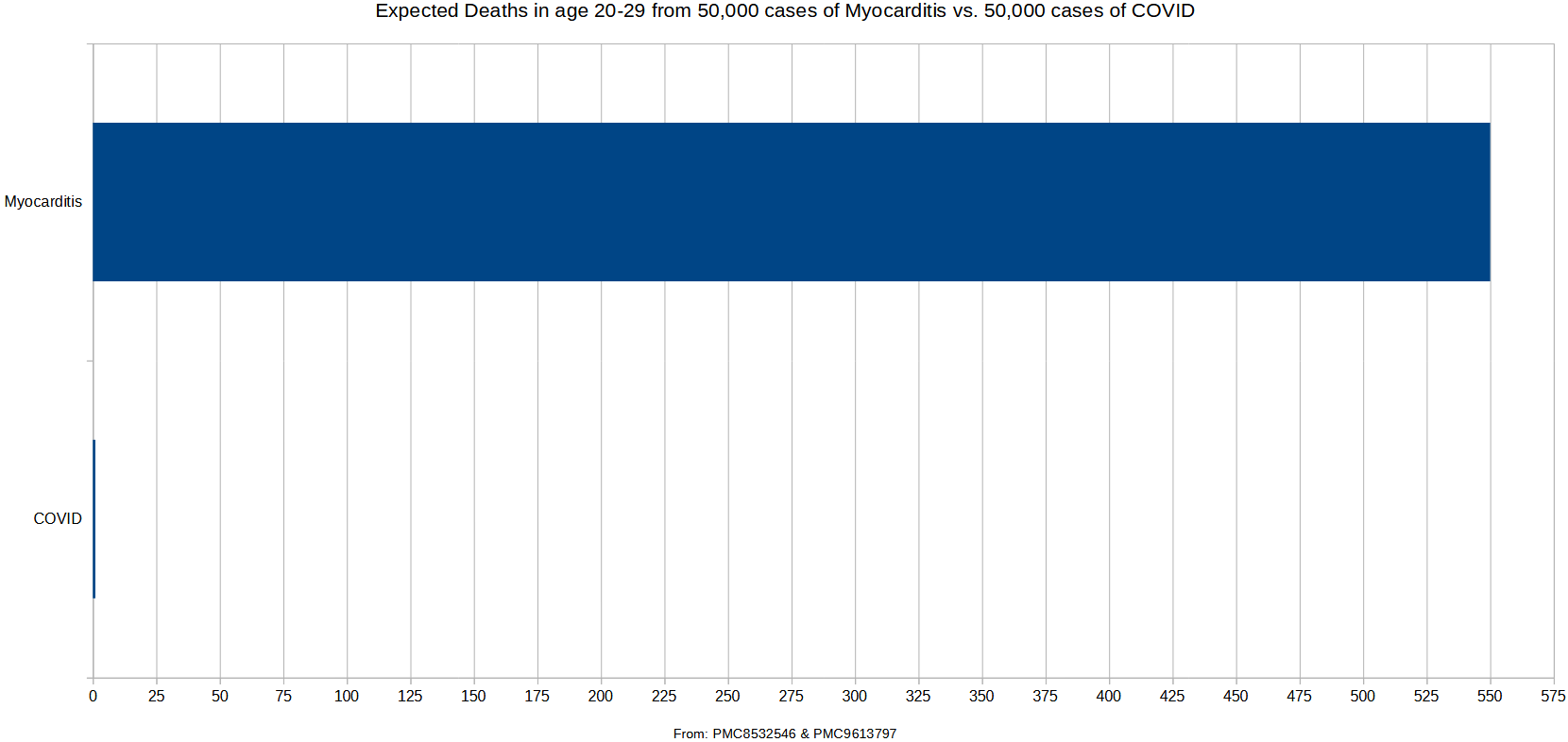
As you can see, myocarditis for those in their 20’s is 550 times more fatal than COVID is for them. But when the risk of death-by-myocarditis is compared to the risk of death-by-COVID for all those under age 20 — then the COVID shots most-clearly offer net-negative benefit.
Because the risk of death-by-myocarditis for them is 3,700 times higher than the risk of death-by-COVID — then if a case of myocarditis is caused before 3,700 cases of COVID are prevented by the COVID shots, then you will get net harm. Hong Kong data extrapolate to a “caused myocarditis case” for every 3,200 doses or so.
If you cannot prevent 3,700 COVID cases with less than 3,200 doses of COVID shots (~116% vaccine efficacy), then the COVID shot for this age band is a non-starter. Evidence suggests that COVID shots for those under age 20 do not even remotely make medical sense, as Hong Kong data indicate more harm than good (net harm).
Reference
Pezzullo AM, Axfors C, Contopoulos-Ioannidis DG, Apostolatos A, Ioannidis JPA. Age-stratified infection fatality rate of COVID-19 in the non-elderly population. Environ Res. 2023 Jan 1;216(Pt 3):114655. doi: 10.1016/j.envres.2022.114655. Epub 2022 Oct 28. PMID: 36341800; PMCID: PMC9613797. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9613797/
Lin YC, Chang CH, Su WJ, Yang CH, Wang JT. Risk of Coronavirus Disease 2019 Messenger RNA Vaccination-Associated Myocarditis and Pericarditis - A Systematic Review of Population-Based Data. Risk Manag Healthc Policy. 2023 Oct 9;16:2085-2099. doi: 10.2147/RMHP.S422372. PMID: 37841076; PMCID: PMC10575036. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10575036/
Kragholm KH, Lindgren FL, Zaremba T, Freeman P, Andersen NH, Riahi S, Pareek M, Køber L, Torp-Pedersen C, Søgaard P, Hagendorff A, Tayal B. Mortality and ventricular arrhythmia after acute myocarditis: a nationwide registry-based follow-up study. Open Heart. 2021 Oct;8(2):e001806. doi: 10.1136/openhrt-2021-001806. PMID: 34675133; PMCID: PMC8532546. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8532546/