

Rare Diseases

COVID shots are associated with high rates of adverse events, such as being associated with Heavy Menstrual Bleeding at over 300 times the rate of typical vaccines. VAERS was checked for a few rare diseases, those with a prevalence of less than 3 persons per million, or those with yearly incidence of under 1 per million.
Lymphangioleiomyomatosis (“limf-AN-gee-oh-ly-oh-my-oh-muh-TOH-sis”) is a rare disorder where cysts grow in your lungs, kidneys, and lymphatic system — often producing shortness of breath and chest pain and cough. The prevalence is about 2.5 persons per million (almost all female) and yearly incidence is 0.135 per million:
Starting off with 230 million people dosed with COVID shots by March 2023 …
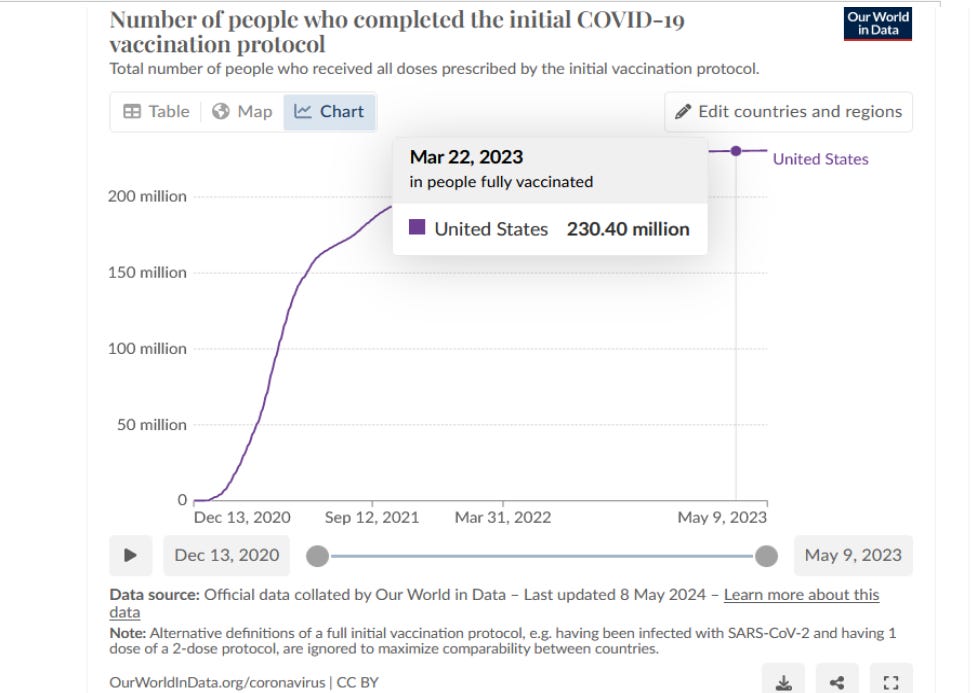
… and assuming that, by then, the average time they had spent fully-jabbed had been 1.5 years — then you have 345.6 million person-years of exposure. With a baseline rate of 0.135 cases per million person-years for lymphangioleiomyomatosis, the expected number of new cases would be (345.6 * 0.135 =) 47 of them.
Because the median capture rate for passive surveillance like VAERS is 6% capture of the underlying events which had been occurring in the background, then the expected number of reports is (0.06 * 47 =) 3 reports. Then we check VAERS …
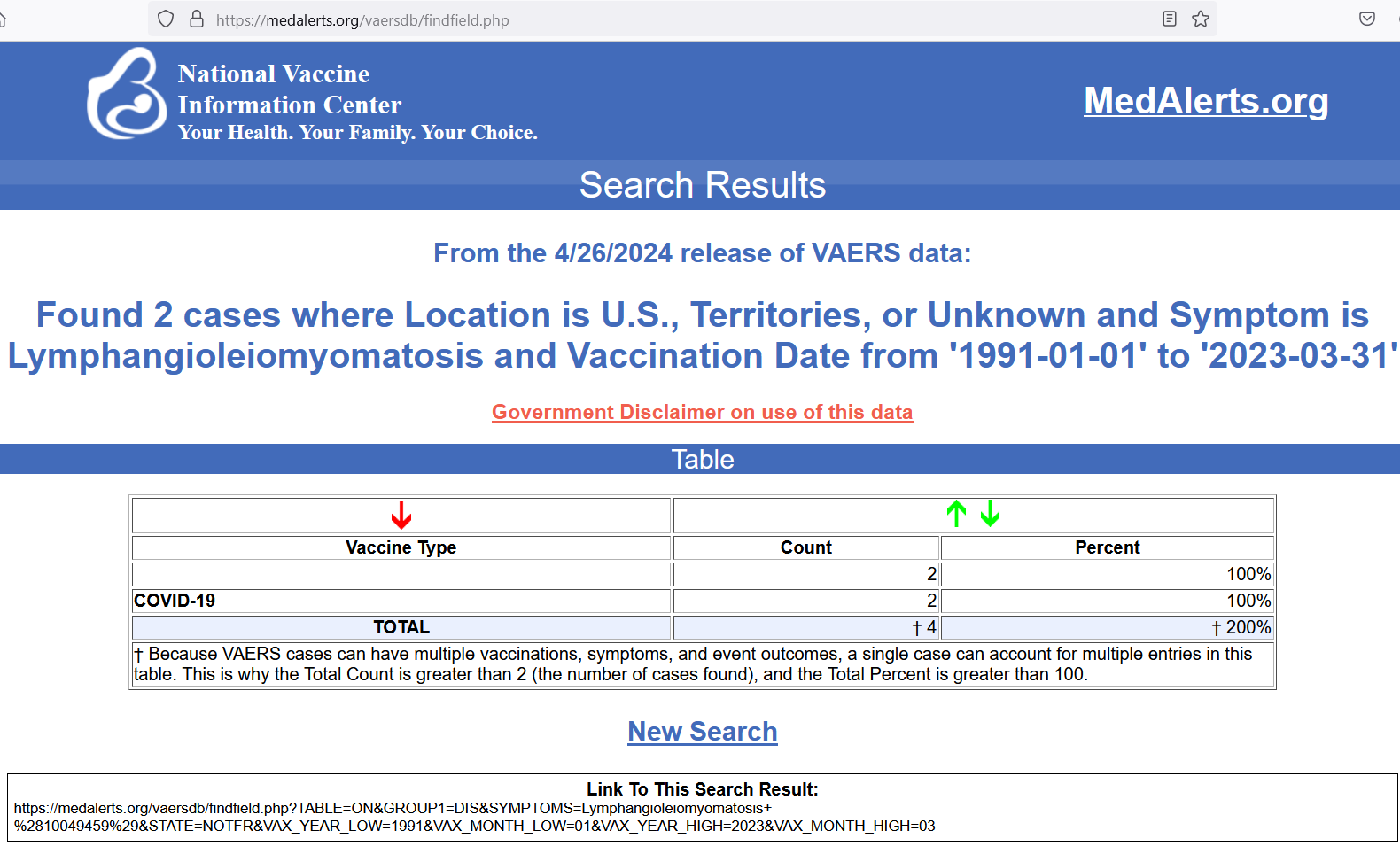
Under the assumptions above, we didn’t find a clear excess of VAERS reports for this rare condition — but if assumptions change by 20% or so, we’d run into numbers which indicate a safety signal for lymphangioleiomyomatosis.
Notice how, even though all other vaccines (~3500 million person-years) had ~10 times the U.S. exposure as the COVID shots (350 million person-years), only COVID shots were linked to lymphangioleiomyomatosis — i.e., not a single report of lymphangioleiomyomatosis for any other vaccine type in 32.25 years of data.
But let’s check a disease (Evan’s syndrome) that is so rare that it has less than half of the prevalence of lymphangioleiomyomatosis — only 1 person per million has it. Evan’s syndrome is an autoimmune condition with 2 or more cytopenias (low counts of blood cell types). A common factor is when IgG antibodies attack red blood cells.
With less than half the cases expected as for lymphangioleiomyomatosis, then that means that less than 1.5 total reports in VAERS are expected for COVID shots. Let’s check VAERS to find out the real number of reports …
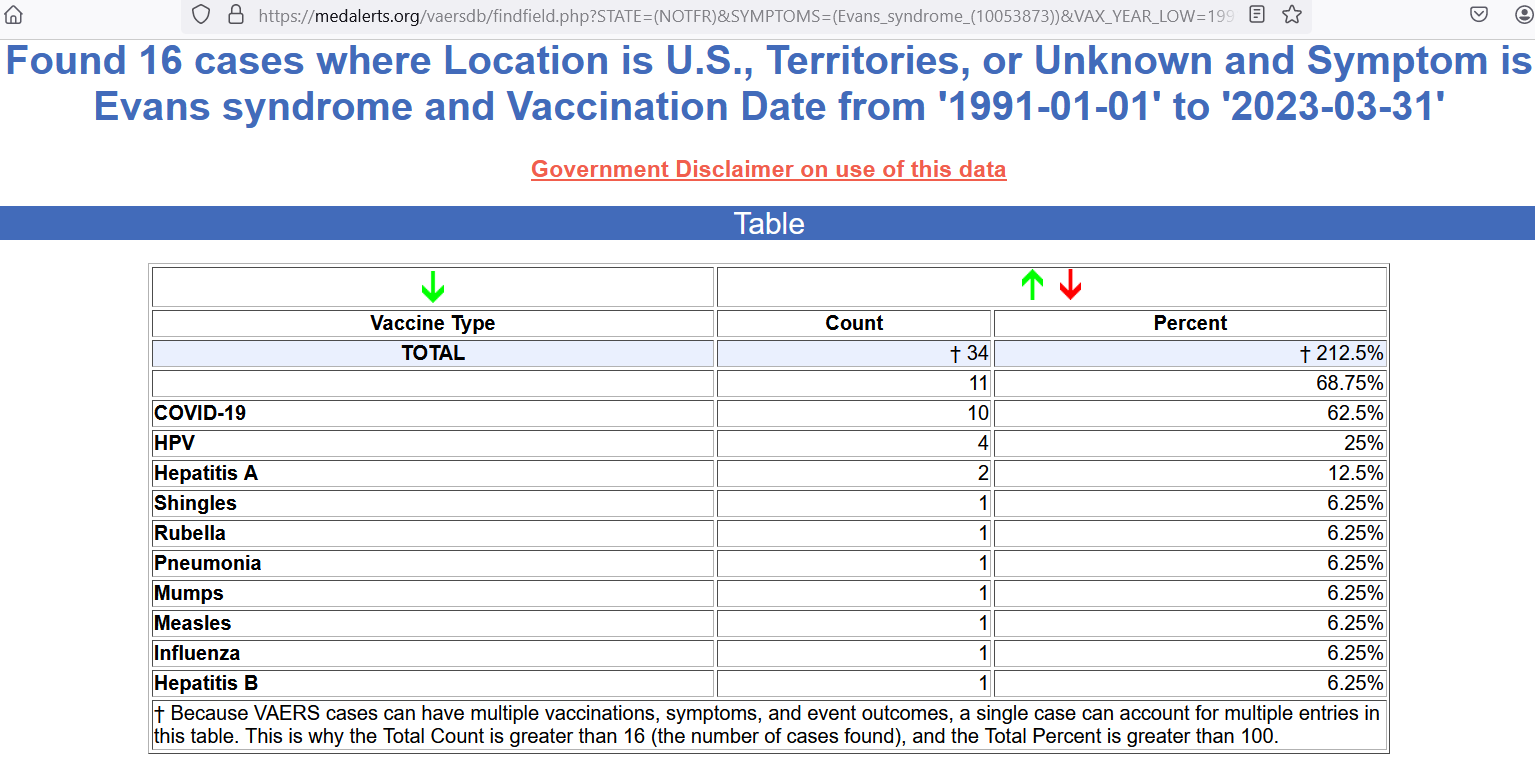
The reports for Evans syndrome in VAERS are 6 times higher than expectations, using the assumptions we’ve laid out above. When the 95% lower bound on the estimate is still 50% above expectations, then it counts as a safety signal. With a central estimate of 10 reports for COVID shots, the 95% lower bound is 4.8 reports — a safety signal.
To get the 95% lower bound on this raw count of events, this Excel formula is used:
=GAMMA.INV(0.025,10,1)
It is the very same formula that CDC uses. The first number means you look for the [2.5]th percentile value, the middle number is the observed count, and the final number represents a parameter set to 1 for these computations. If you copy and paste the formula into Excel, and hit Enter, you’ll get the same result (4.8 lower bound).
Because exceeding expectations by 50% would have been enough, then any lower bound value above 2.25 would have thrown a statistically-significant safety signal. With a 4.8 lower bound, the signal for Evans syndrome from COVID shots is strong. This was something to suspect, because COVID shots create autoimmune issues.
Reference
[list of rare diseases] — https://www.orpha.net/pdfs/orphacom/cahiers/docs/GB/Prevalence_of_rare_diseases_by_decreasing_prevalence_or_cases.pdf
[Evan’s syndrome] — https://www.ncbi.nlm.nih.gov/books/NBK519015
[lymphangioleiomyomatosis] — https://my.clevelandclinic.org/health/diseases/16022-lymphangioleiomyomatosis-lam