

A Million COVID Deaths?
A Million COVID Deaths?
From a disease not even twice as bad as flu??

According to Worldometers, the US COVID death tally passed the “1 million deaths” mark, but this high amount of death is not consistent with robust (n > 100,000 COVID infections) lethality data on COVID.
A tip-off that instrinsic COVID lethality is too low in order to ever be able to cause a million deaths in two years comes from comparing the deaths per million in the US to that of South Korea:

The instrinsic lethality of COVID is something which leads to about 270 deaths per million at the two-year mark (annual death rate of 135 deaths per million), as indicated by COVID death data in South Korea.
But the US is almost up to 3000 deaths per million at the two-year mark (almost an annual death rate of 1500 deaths per million) — over 10 times the COVID death rate of South Korea. A major difference between the US and South Korea is the date when each nation reached a threshold of 60 vaccine doses administered per 100 people.
A vaccine uptake level of about 60 doses per 100 is associated with excess mortality, as most nations had excess mortality as they crossed that threshold of vaccine uptake. Indeed, it is hard to find nations which did NOT have excess mortality as they crossed that threshold of vaccine uptake.
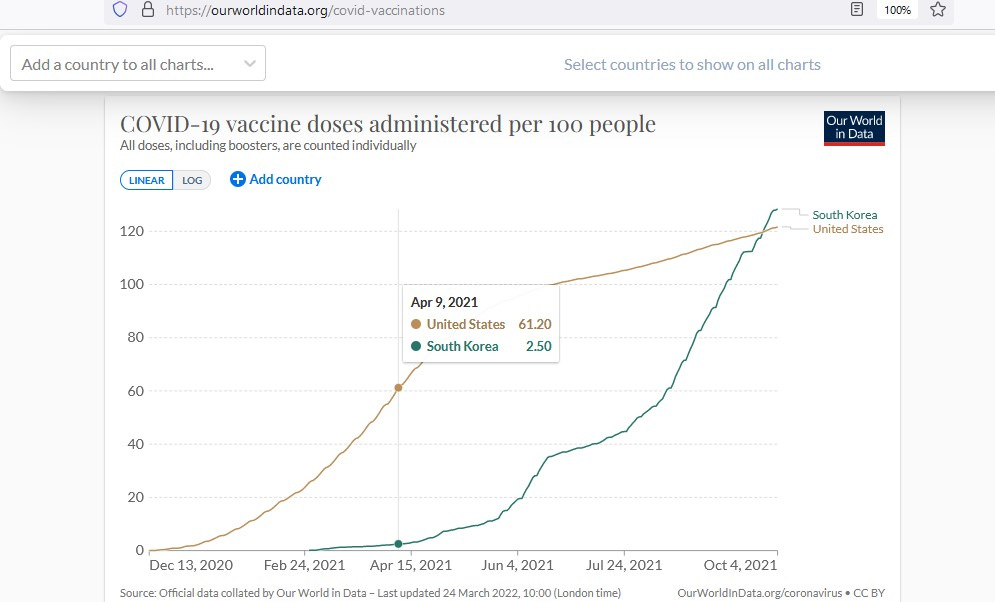
While the US reached this mark by 9 Apr 2021, South Korea didn’t administer 60 doses per 100 people until 13 Aug 2021 — a full 126 days after the US did.
With 4 months less exposure to this ‘moderate’ vaccine uptake level than the US, South Korea may have had an advantage over the US — under the assumption that vaccine-mediated enhanced disease (VMED) plays a role in the million deaths found in the US.
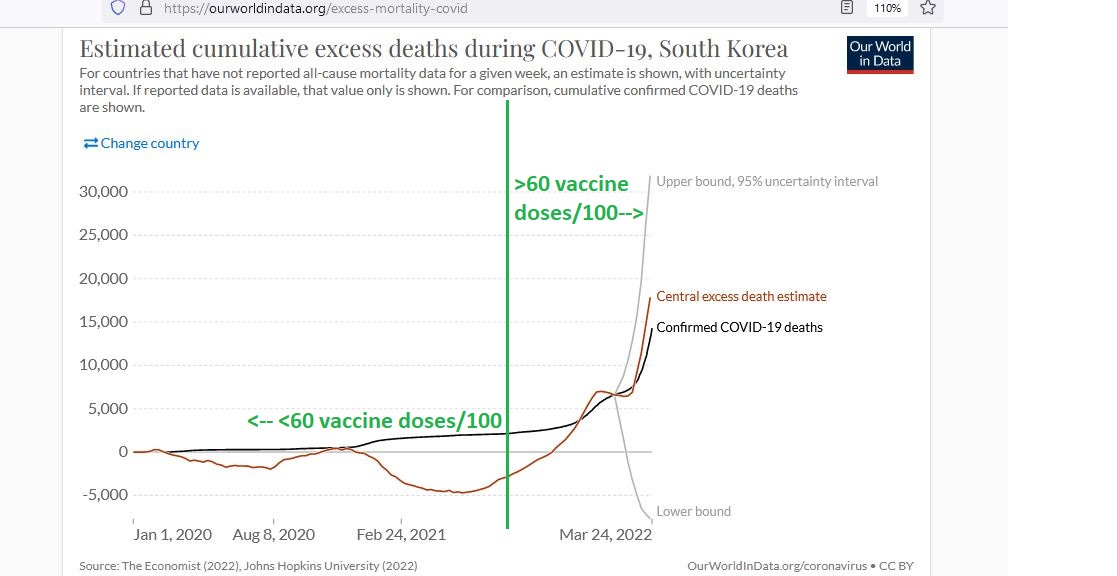
Being 4 months ahead of South Korea by this vaccine measure may have helped lead the US to having more than 10 times the COVID death. Here is a graph of South Korea showing what happened to them as they crossed the critical threshold of 60 vaccine doses per 100 people:
The Intrinsic Lethality of COVID Variants
The intrinsic lethality of COVID variants has stepped down over time, though it is possible that the Alpha variant was an exception, and that it alone led to a step-up in COVID lethality of around 30% to 40% higher than wild-type (“Wuhan-1”) COVID.
While Alpha variant dominance coincided with winter, so that some of the excess fatality would be expected from the expected reduction in levels of vitamin D, it still does appear that Alpha was about a third more lethal than wild-type COVID:

The table above shows the median age of COVID deaths was above 80 in an eastern region of England. Case fatality for wild-type COVID had come down by two-thirds by May of 2020, after a dramatic shrinking of the cohort with the least immunity to COVID, during the first two months of March and April.
As Autumn set in and vitamin D levels began dropping, wild-type COVID case fatality rates rose again, from 9.9% up to 17.3%. By 4 Jan 2021, Alpha variant was the dominant COVID variant in circulation, and deaths ran about 50% to 60% higher than wild-type COVID deaths.
But some of that fatality increase is due to lowered vitamin D levels and not to intrinsic COVID lethality, and some of it may even be due to uptake of vaccines. A residual of about 30% or so may be best explained by Alpha variant being the most-lethal COVID variant ever seen throughout the entire multi-year pandemic.
To estimate the lethality of early (pre-Delta variant) COVID, including this most-lethal-of-all-COVID-variants (Alpha), I formed a 99% credible interval around COVID death data for 117,000 COVID cases followed through time, so as to estimate the infection fatality rate (IFR).
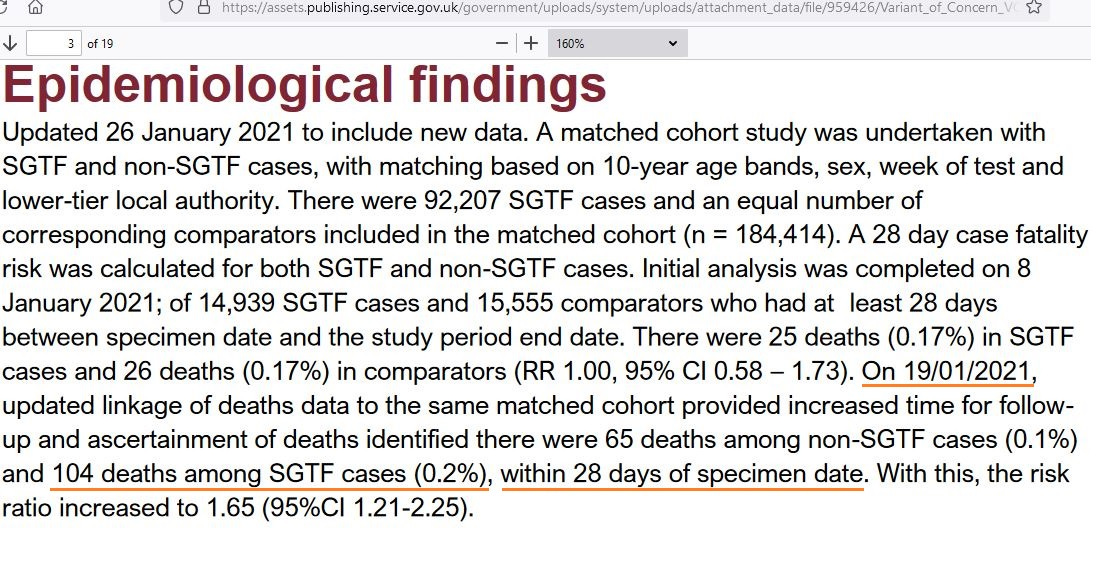
First, here are the official death statistics on 117,000 COVID cases followed through time, leading to 169 total deaths — 104 of which were Alpha variant cases, as identified by S-gene target failure (SGTF):
And here is the 99% Bayesian credible interval showing both the most-likely COVID IFR, and the bounds of plausibility on a COVID IFR:

As you can see, the combination of COVID variants circulating by the end of 2020 had led to a most-likely IFR of 0.146% — which is statistically equivalent to the 0.148% IFR for the flu season of 2010/11. The 99% upper bound of plausibility for a pre-Delta COVID IFR was 0.176% — which is about 60% worse than the average seasonal flu.
It’s difficult to imagine getting a million deaths from a disease that is not even twice as bad as flu, though.
Let’s look just at the most-lethal-of-all-COVID-variants (Alpha) and get plausibility limits on its lethality, to see if it was something that could possibly cause a million deaths in the US alone:

The most likely IFR on this most-lethal-of-all-COVID-variants (Alpha) is 0.2% — the same estimate found by the UK Technical Briefing #5 quoted above. This IFR estimate on this worst-ever-COVID-variant is still only 80% worse than flu though.
Even the worst-ever COVID variant was not even twice as bad as flu.
How Does a Million Deaths in Two Years get Explained then?
You can’t get a million deaths from something that is not even twice as bad as flu, so we will have to look beyond COVID to explain the COVID deaths (COVID isn’t lethal enough to be able to cause the COVID deaths).
Considering the order-of-magnitude difference in death data found between the US and South Korea — two nations which were at extreme ends regarding the time it took to get 60 vaccine doses administered per 100 people — a likely explanation is vaccine-mediated enhanced disease (VMED).
While COVID isn’t deadly enough to be able to explain a million COVID deaths, if it had “help” from vaccines enhancing it, then the million COVID deaths might finally get explained.
Reference
[Fraction of flu infections with symptoms = 84%] — Leung NH, Xu C, Ip DK, Cowling BJ. Review Article: The Fraction of Influenza Virus Infections That Are Asymptomatic: A Systematic Review and Meta-analysis. Epidemiology. 2015 Nov;26(6):862-72. doi: 10.1097/EDE.0000000000000340. PMID: 26133025; PMCID: PMC4586318. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4586318/
[Avg. flu IFR from Fall of 2012 to Spring of 2019 = 0.11% (after adjusting symptomatic cases by dividing by 0.84, the background fraction of all flu infections which have symptoms] — CDC Burden of Flu data. Available: https://www.cdc.gov/flu/about/burden/index.html
[Alpha variant was likely about a third more lethal than Wild-type COVID] — Brainard J, Grossi Sampedro CM, Sweeting A, Fordham R. Was Alpha deadlier than wild-type COVID? Analysis in rural England. Infection. 2022 Mar 5:1–8. doi: 10.1007/s15010-022-01787-x. Epub ahead of print. PMID: 35247164; PMCID: PMC8898029. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8898029/
[As of 19 Jan 2021, from about 117,000 COVID infections, there were 169 total deaths (IFR=0.144%)] — UK Technical Briefing #5. Available general: https://www.gov.uk/government/publications/investigation-of-novel-sars-cov-2-variant-variant-of-concern-20201201
Available specific page: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/959426/Variant_of_Concern_VOC_202012_01_Technical_Briefing_5.pdf