
Benchmark Infection Fatality Rates
Age-based benchmarking

To figure out if poor medical care has been given, you have to have a benchmark on the background infection fatality rate (IFR) for a disease.
While medical cases (those typically seen in hospital) are typically more severe than infections overall, if the age-based mortality rate after treatment veers “very far” from the benchmark infection fatality rate, then it indicates that poor medical care was given out.
Caveat: While the phrase “very far” is admittedly subjective, most concerned onlookers would be alarmed if age-based death rates were higher by an order of magnitude above benchmark infection fatality rates.
Updated age-based IFRs were published online in Oct of 2022, and you can use a stepping-down process on the IFR of the original strain of COVID in order to find the IFR of Delta variant.
You can then use a stepping-down process on the IFR of Delta variant to get to the IFR of Omicron variant.
Why an IFR Step-Down is preferred to real-time estimates
This method of IFR estimation is preferable to real-time estimation because real-time estimates of Delta and Omicron will all include the confounding variable of experimental COVID injections.
If an experimental injection has been given, you can’t tell if the infection fatality rate estimate represents the disease or the effect of the “treatment.” But if you compare a mix of injected people and uninjected people across variants, while the absolute value may be higher (due to the share of people injected or not), the relative drop should still be realistic.
The step-down should still capture the underlying relative fatality.
When this process is performed on the October 2022 estimates, you get the following graph for age-based original strain IFR versus Omicron variant IFR:
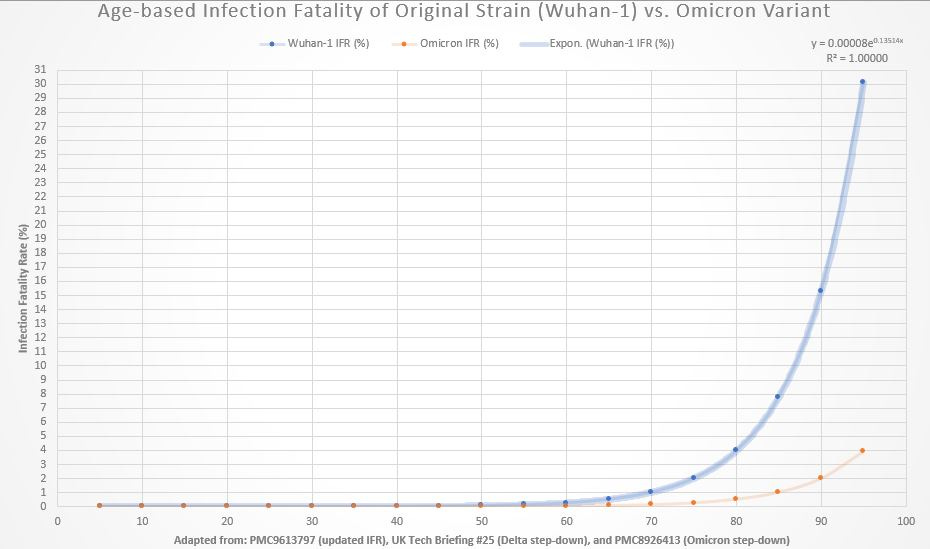
The age-based IFR model is an exponential model using median age-bracket values for those below age 70 — and projecting from that fitted model up to age 95. To find out if too many people in an age bracket have been dying — possibly due to poor medical care — here is the same graph with notes at IFR values of 1% and 4%:
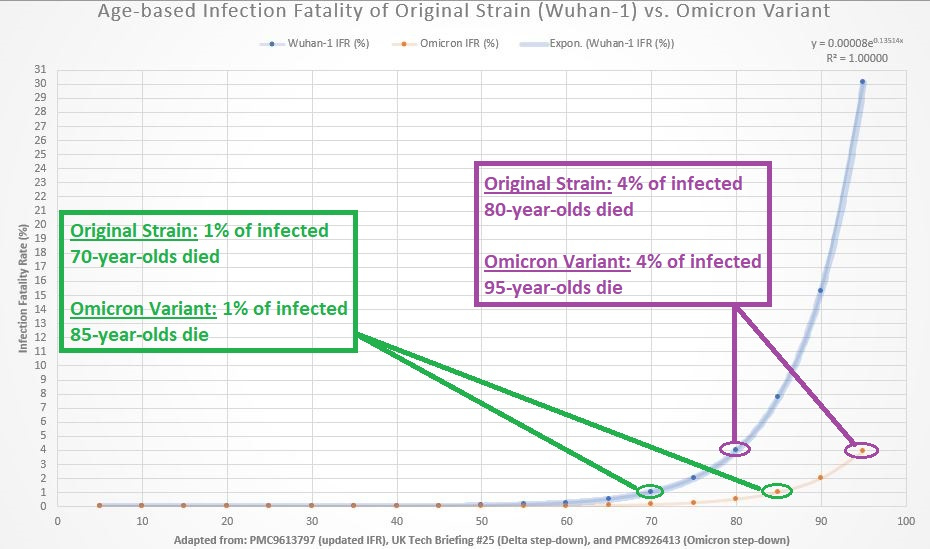
Notice how Omicron shifted the fatality curve by 15 years.
End Notes:
To get the original IFR in percentage form for any individual age, use this formula:
IFR(%) = 0.00008 * e^0.13514*(age in years)
That’s the function which fitted the original strain median IFR estimates the best. After obtaining the original strain IFR, convert to Omicron by multiplying it by 0.1302 — or simply use the converted form of the function for Omicron:
IFR(%) = 0.00001 * e^0.13514*(age in years)
Reference
[true IFR of Wuhan-1 COVID] — Pezzullo AM, Axfors C, Contopoulos-Ioannidis DG, Apostolatos A, Ioannidis JPA. Age-stratified infection fatality rate of COVID-19 in the non-elderly population. Environ Res. 2023 Jan 1;216(Pt 3):114655. doi: 10.1016/j.envres.2022.114655. Epub 2022 Oct 28. PMID: 36341800; PMCID: PMC9613797. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9613797/
[IFR step-down to Delta (42% as fatal as prior variants; sequenced cases only)] — Table 3; sequenced cases only (n ~ 700,000). Number of confirmed and probable cases by variant as of 11 October 2021. UK Technical Briefing #25. https://www.gov.uk/government/publications/investigation-of-sars-cov-2-variants-technical-briefings
[IFR step-down from Delta to Omicron (31% as fatal as Delta)] — Nyberg T, Ferguson NM, Nash SG, Webster HH, Flaxman S, Andrews N, Hinsley W, Bernal JL, Kall M, Bhatt S, Blomquist P, Zaidi A, Volz E, Aziz NA, Harman K, Funk S, Abbott S; COVID-19 Genomics UK (COG-UK) consortium, Hope R, Charlett A, Chand M, Ghani AC, Seaman SR, Dabrera G, De Angelis D, Presanis AM, Thelwall S. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022 Mar 16:S0140-6736(22)00462-7. doi: 10.1016/S0140-6736(22)00462-7. Epub ahead of print. PMID: 35305296; PMCID: PMC8926413. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8926413/