


COVID Shots for those under Age 50
Post #1062

Health officials and bureaucrats have been relying on modeling studies in order to rationalize the use of COVID shots. One of the most-frequently cited studies said this:
“Based on official reported COVID-19 deaths, we estimated that vaccinations prevented 14·4 million (95% credible interval [Crl] 13·7–15·9) deaths from COVID-19 in 185 countries and territories between Dec 8, 2020, and Dec 8, 2021.”
But an alternative to such abstract modeling is to look at the real world, to make sure the numbers pass “the sniff test.” In the real world, COVID deaths over the course of 42 days were tracked in ~600,000 unjabbed people in Israel, and it was found that 32 deaths occurred in 42 days. The reported deaths in those taking the shots was 9 deaths:
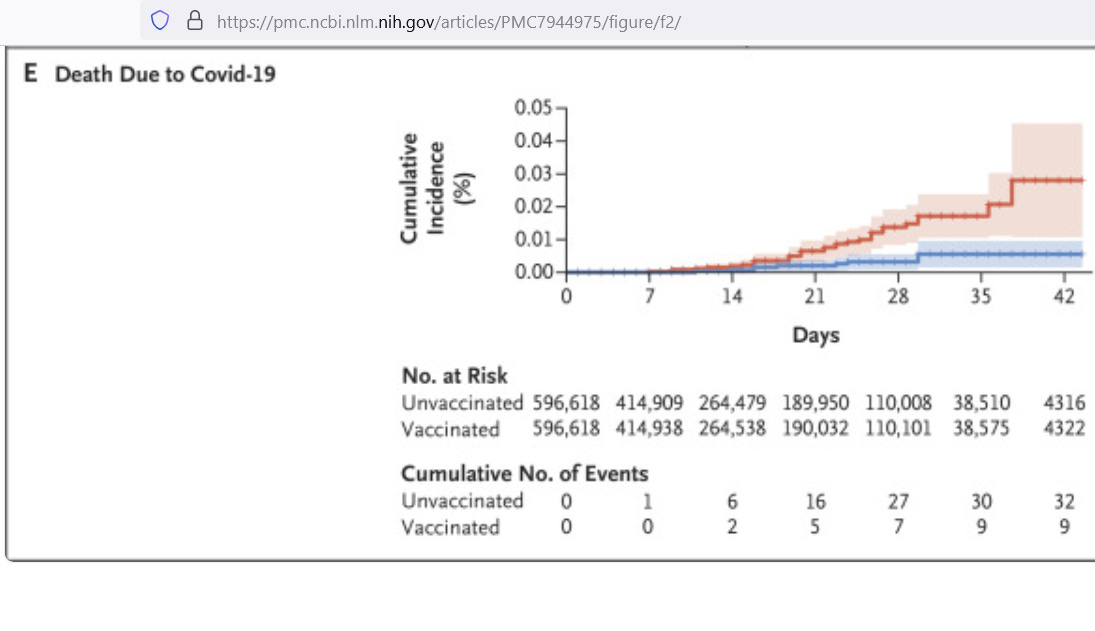
Because 42 days is 11.5% (0.115) of a year, the person-years of observation is
596,618 * 0.115 =
68,611 person-years of observation
With 32 deaths happening inside of those 68,611 person-years, the annualized COVID death rate (per 100,000) for unjabbed people would be
32 / 0.68611 =
46.6 COVID deaths per 100,000
But that death rate isn’t much higher than the top death rate found in Italy for seasonal influenza when it was tracked over the course of 4 flu seasons:
“The average annual mortality excess rate per 100,000 ranged from 11.6 to 41.2 with most of the influenza-associated deaths per year registered among the elderly. "
This indicates that COVID wasn’t much more dangerous than a bad flu. And when you actually take the difference in deaths between jabbed and unjabbed — because it is that number that was actually modeled — you get 33.5 deaths averted per 100,000 per year. That rate of prevention is definitely within recorded numbers for flu deaths.
In other words, if you believe the model up top, then you must also believe that seasonal flu can cause 14.4 million deaths in a year — based off of the prevention rate found in the real world experience of Israel. While the numbers do not add up, even worse is what happened to those under age 50. CDC numbers show limited efficacy:
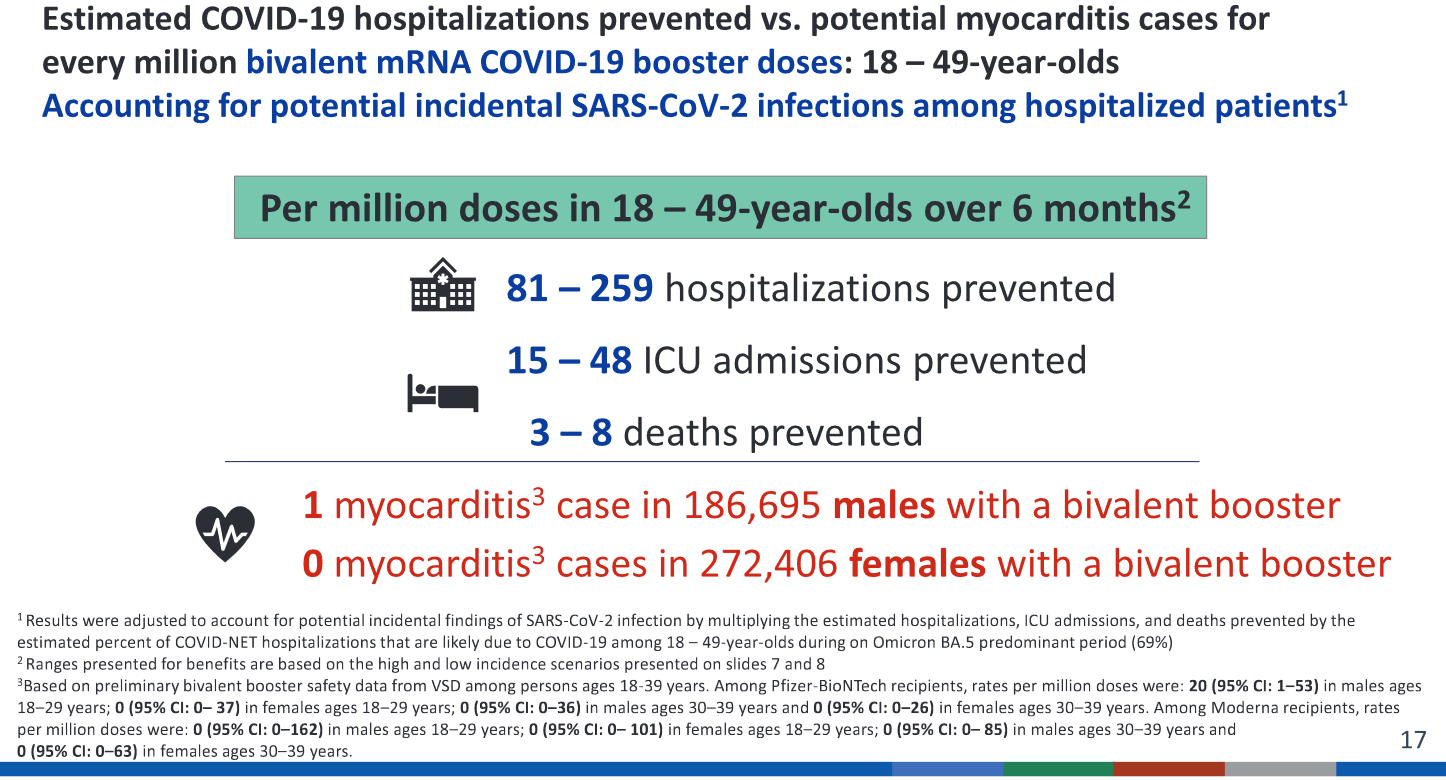
At only up to 259 hospitalizations prevented per million doses, and only up to 8 deaths prevented, these numbers do not look good when compared to adjusted VAERS death reports. Before showing them though, the worst protocol decisions were to give COVID shots to teens or younger:
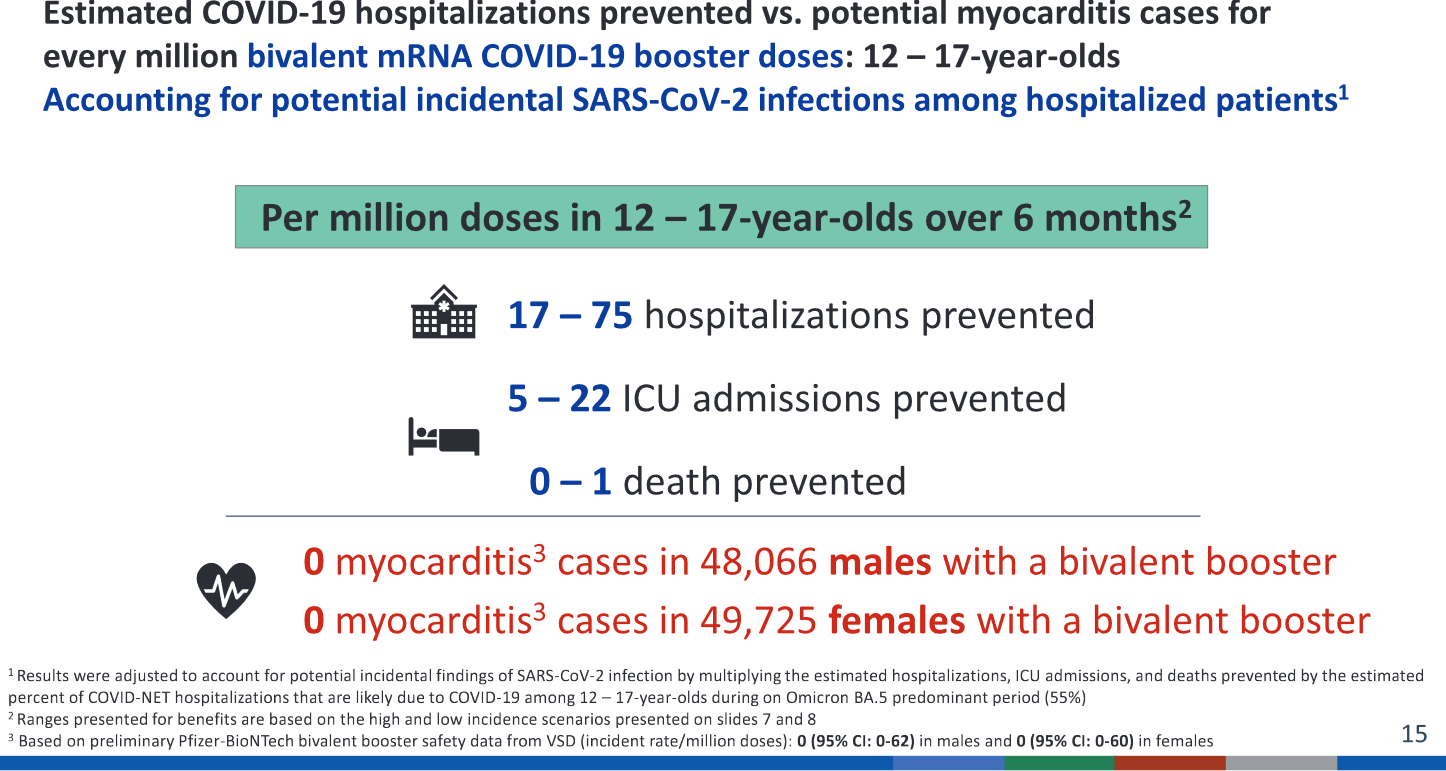
With only up to 75 hospitalizations prevented per million doses, and only up to 1 death prevented, there is a clear negative benefit-harm effect just from myocarditis alone. By the time you have prevented 75 COVID hospitalizations from giving a million doses, you have also caused up to 146.1 cases of myocarditis in teen males:
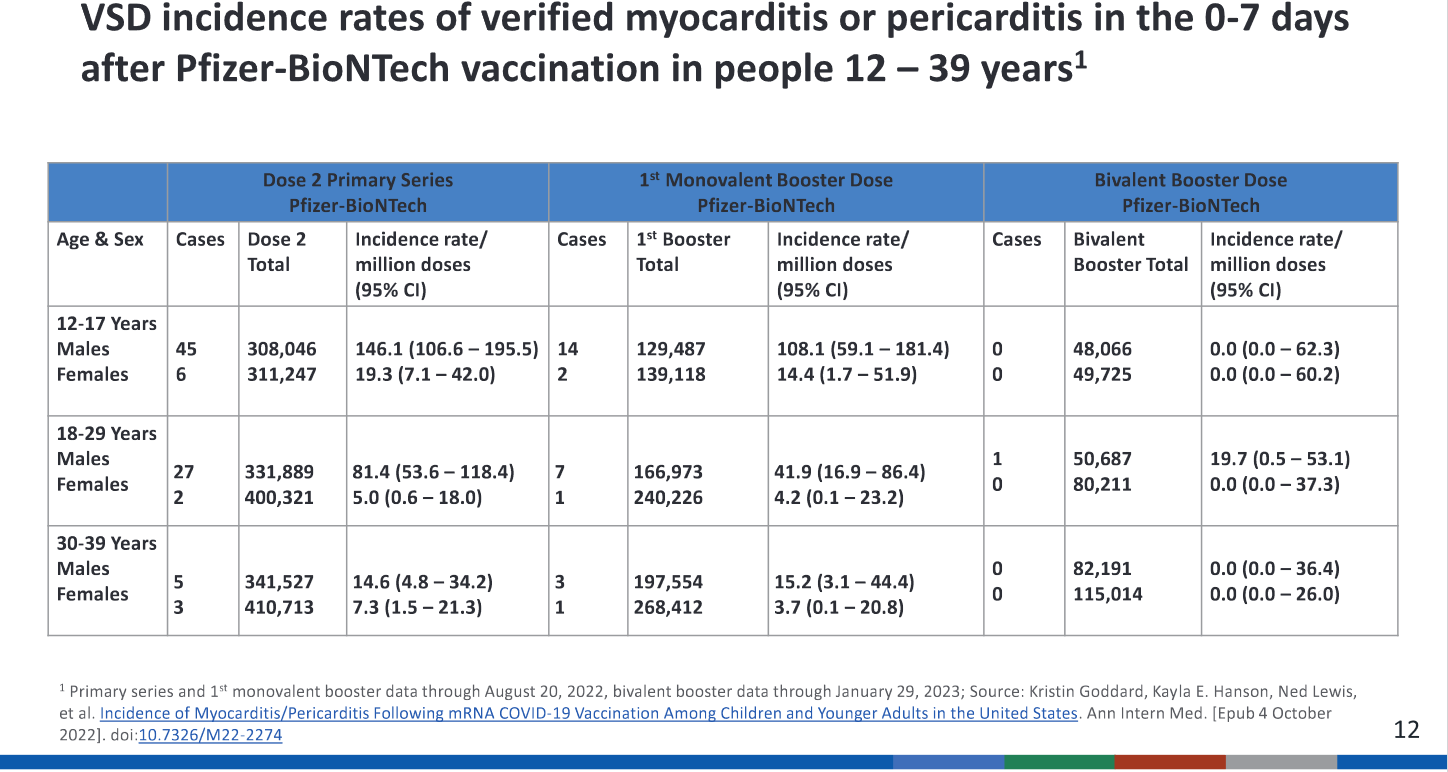
The 90-day death rate from induced myocarditis is around 1% (146 cases => ~1.46 deaths), so even the death data do not come down on the side of the COVID shots. Now let’s look at the situation that those under age 50 face. CDC says that up to 8 deaths can be prevented by giving a million shots to them, but here’s Moderna’s VAERS reports:
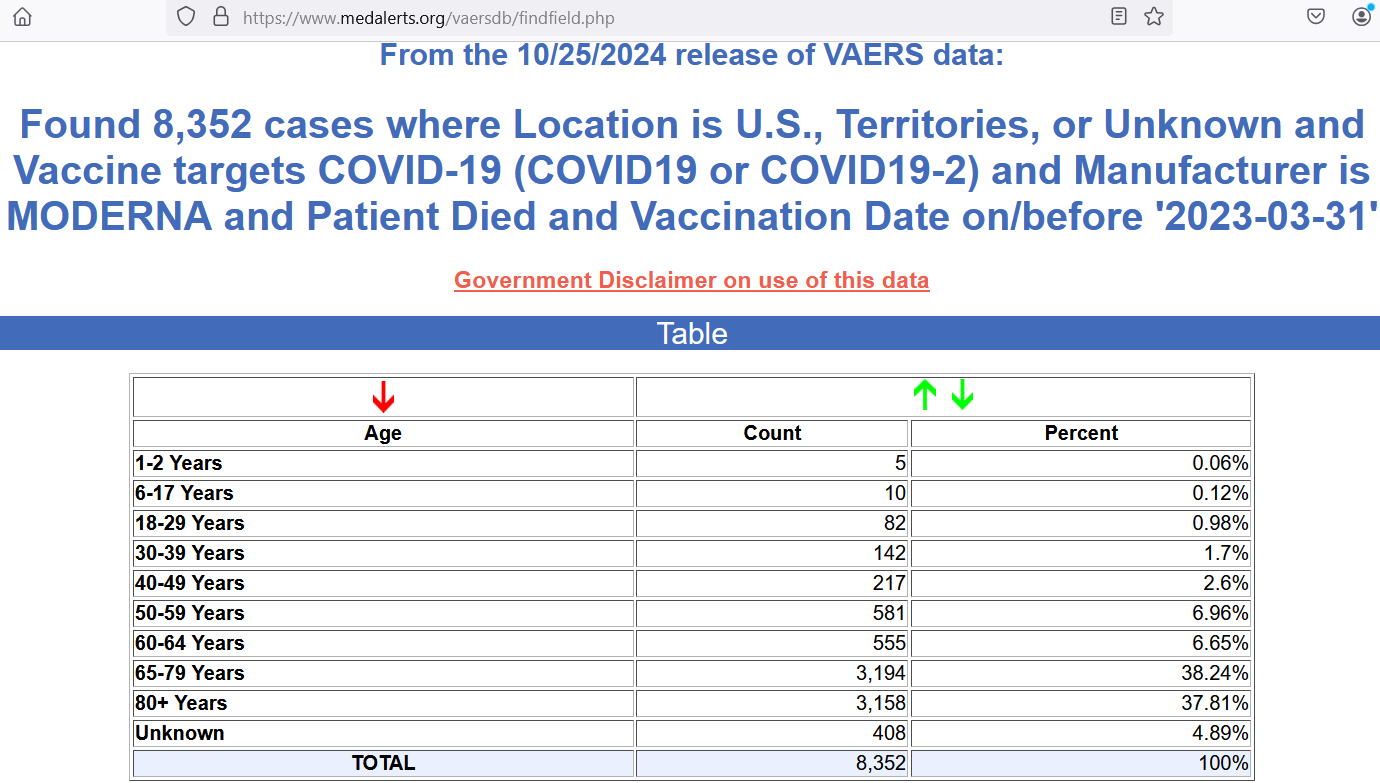
Because it runs to the end of March 2023, you can work out the death reports per million doses. There had been 251.85 million Moderna doses given by then, making for a reporting rate of
8352 / 251.85 =
33.2 reports of death per million doses
That number involves all ages though, so it isn’t clear if it shows net harm yet — because the age group that we’re examining is under age 50 — and that group only had from 456 to 864 VAERS death reports by March 2023. This means that they represent from 5% to 10% of the total deaths reported to VAERS.
But I don’t have COVID shot uptake levels for that age group only, so let’s carry the all-ages analysis forward and then adjust it down at the end. We still need to factor in the rate of under-reporting.
The median rate of underreporting is 94%, meaning that only about 6% of the background events are making into the VAERS system, and 94% of them never make it into VAERS. When 6% of actual events make it in, you must multiply reports by 16.7 to estimate what is happening in the background. This brings Moderna deaths to 139,200.
And it brings the imputed Moderna shot death rate (MSDR) to 553 deaths per million doses. That’s a death for every 1,800 doses given out, but it is 69 times higher than the deaths averted by the COVID shots for those under age 50 (according to CDC). Even if you assume that those under 50 have a rate that is only 5% of that, you get:
553 * 0.05 =
28 deaths in those under age 50 per million doses
That’s still over 3 times higher than the number of COVID deaths averted (using CDC’s numbers). But who, in their right mind, would want to use an injectable compound that causes at least 3 deaths for every death that it purportedly prevents?
Reference
[model showing 14.4 million COVID deaths averted in a single year] — Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis. 2022 Sep;22(9):1293-1302. doi: 10.1016/S1473-3099(22)00320-6. Epub 2022 Jun 23. Erratum in: Lancet Infect Dis. 2023 Oct;23(10):e400. doi: 10.1016/S1473-3099(23)00566-2. PMID: 35753318; PMCID: PMC9225255.
[real world study showing an annualized COVID death rate of 46.4 COVID deaths per 100,000] — Dagan N, Barda N, Kepten E, Miron O, Perchik S, Katz MA, Hernán MA, Lipsitch M, Reis B, Balicer RD. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N Engl J Med. 2021 Apr 15;384(15):1412-1423. doi: 10.1056/NEJMoa2101765. Epub 2021 Feb 24. PMID: 33626250; PMCID: PMC7944975. https://pmc.ncbi.nlm.nih.gov/articles/PMC7944975/
[flu death rate up to 41.2 per 100,000 in Italy] — Rosano A, Bella A, Gesualdo F, Acampora A, Pezzotti P, Marchetti S, Ricciardi W, Rizzo C. Investigating the impact of influenza on excess mortality in all ages in Italy during recent seasons (2013/14-2016/17 seasons). Int J Infect Dis. 2019 Nov;88:127-134. doi: 10.1016/j.ijid.2019.08.003. Epub 2019 Aug 8. PMID: 31401203. https://www.ijidonline.com/article/S1201-9712(19)30328-5/fulltext
[number of hospitalizations and deaths prevented by a million doses] — Benefit and risk assessment for COVID-19 vaccines. February 24, 2022. By Wallace, Megan. Series: ACIP meeting COVID-19 Vaccines. https://stacks.cdc.gov/view/cdc/125169
[90-day death rate from jab-induced myocarditis was 1.0%] — Lee YK, Kwon Y, Heo Y, Kim EK, Kim SY, Cho H, Kim S, Ko M, Lim D, Seo SY, Cho E. Safety monitoring of COVID-19 vaccines: February 26, 2021, To June 4, 2022, Republic of Korea. Clin Exp Pediatr. 2023 Oct;66(10):415-423. doi: 10.3345/cep.2022.00815. Epub 2023 Jun 13. PMID: 37309116; PMCID: PMC10556797. https://pubmed.ncbi.nlm.nih.gov/37309116/
[90-day death rate from jab-induced myocarditis was 1.1%] — Husby A, Gulseth HL, Hovi P, Hansen JV, Pihlström N, Gunnes N, Härkänen T, Dahl J, Karlstad Ø, Heliö T, Køber L, Ljung R, Hviid A. Clinical outcomes of myocarditis after SARS-CoV-2 mRNA vaccination in four Nordic countries: population based cohort study. BMJ Med. 2023 Feb 1;2(1):e000373. doi: 10.1136/bmjmed-2022-000373. PMID: 36936260; PMCID: PMC9978676. https://pubmed.ncbi.nlm.nih.gov/36936260/
[251.85 million Moderna doses in USA by 22 Mar 2023] — OWID. https://ourworldindata.org/covid-vaccinations
[8,352 Moderna death reports to VAERS in USA up to March 2023] — MedAlerts. https://www.medalerts.org/vaersdb/findfield.php
[median under-reporting rate of 94% = 6% capture rate] — Hazell L, Shakir SA. Under-reporting of adverse drug reactions : a systematic review. Drug Saf. 2006;29(5):385-96. doi: 10.2165/00002018-200629050-00003. PMID: 16689555. https://pubmed.ncbi.nlm.nih.gov/16689555/