

Dr. Nass' Medical Hearing
Dr. Nass' Medical Hearing
Expert witness caught "over-testifying"

Dr. Meryl Nass has been put through an excruciating medical hearing by the Medical Board of Maine. One of the expert witnesses present (at least in the 3rd episode of this ‘excruciatingness’) is Dr. Thomas Courtney of the Maine Medical Center. An excellent rejoinder to the witnesses speaking out against Dr. Nass is found at The Defender.
Before piling on about something that Dr. Courtney felt it reasonable to say, I want to express cautious sympathy in that he did not look comfortable witnessing against Dr. Nass and the conspiracy side of my brain suggests he was under duress by the establishment.
Here is the link to the 3rd episode of ‘excruciatingness’ and at Minute Mark 27:20 you will hear a question about an ivermectin prescription by Dr. Nass on 28 Sep 2021. Here is the quote of what Dr. Courtney says:
At this point in time, we knew that ivermectin was not an effective treatment for prevention or treatment of COVID-19.
I’ll give you a few minutes to get your composure after reading that. The nice thing about having the opposition on record is that you can nit-pick what they say. In this sentence from Dr. Courtney, it will be revealed below that there is much hypocrisy.
What it takes to “know” something
Philosophers such as Aristotle were masters at knowing. Not because they were especially smart, but because they were intellectually honest. Intellectual honesty involves knowing what you do and do not know, at any given point in time.
If someone says that round squares do not exist, that would be something about which it is impossible to be wrong. Therefore, it is true knowledge, in the fullest sense of the term, to say that there are no round squares — there never has been, and there never will be round squares.
At one notch down from the immediately self-evident truth of no round squares, is the not-as-immediate self-evident truth available to those who search for it. If someone said they rolled normal casino dice and it came out as a “13” — we know they are lying.
We may not immediately know, like we do when someone says they found a round square, but critical thinking reveals we do know — and that it is impossible for us to be wrong about that.
At another notch down from the self-evident truths only known by thinking well, would be most of the inferences made in the sciences.
How science works
Science, including medical science, works mostly by removing untruths, rather than uncovering truths. Statistics are utilized to get yourself into the position of removing things that have such a small chance of being true, that they are implausible.
On the standard of science, did Dr. Courtney “know what he was talking about” when he declared in Minute 27 that it was “known” that ivermectin was not effective? I think you know the answer to that. A good tool to remove untruths is the confidence interval.
Confidence Intervals
The confidence interval helps you to see two things: magnitude of effect and precision of the estimate. Something could seem really helpful, but have so little data backing it that the confidence interval is wide enough to encompass the possibility of it turning out being harmful.
If I tell you I have magic fairy dust that makes coin flips come out heads, you may ask for an experiment. After applying my magic fairy dust to the coin, and after flipping it three times, it comes out heads all three times.
That’s 100% heads and represents a very large magnitude of effect until you ask how wide the margin of error is on the effect. The 95% lower bound of the interval around the proportion of heads from this coin is still consistent with a coin that only comes up heads 30% of the time!
In other words, even if the coin were unfair in the other direction, coming up tails most of the time, we have not disproven either of these possibilities in our 3 flips of the coin:
the coin is fair, and will come up heads 50% of the time in the long-run
the coin is so unfair that it actually comes up tails 70% of the time
the magical fairy dust is working, and this coin will always come up heads
When using confidence intervals to find out if drugs work, a superiority margin is desired. A superiority margin is a critical threshold for the limit of a confidence interval, put there to help guarantee that the drug or treatment has a defined, clinically-significant benefit compared to placebo or to other drugs.
Here is a forest plot showing different levels of evidence for cardiovascular drugs in preventing composite outcomes including things like heart attacks and strokes (horizontal black lines are 95% confidence intervals):
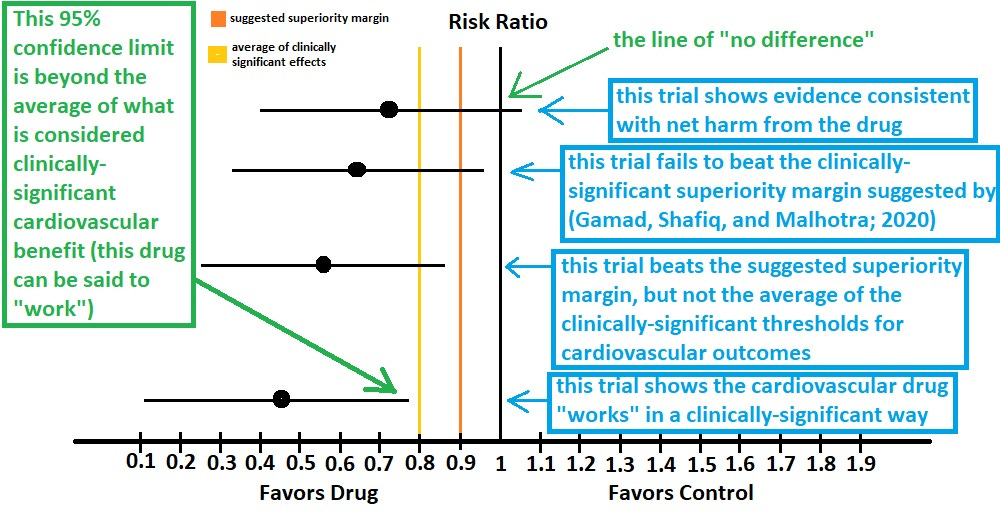
While most drugs get approved by regulatory agencies before reaching the evidence level of the bottom of the plot, we can use the bottom of the plot to represent when we “know” that treatments “work.” Treatments that work are those that cut your risk by more than some minimum amount — by an amount that is deemed to be clinically-significant.
The $64,000 Question
The burning question then becomes this:
If we want to consider ourselves intellectually-honest, do we really know that the established “standard-of-care” for COVID works?
I think you know the answer.
While Dr. Courtney claims to have known that ivermectin doesn’t work against COVID, to turn the tables around on him we can ask: Are those specific things which Dr. Courtney does (or might) recommend for COVID “known” to work?
Masks
One of the standard practices early in the COVID fiasco was for medical doctors to recommend that people walk around wearing cloth or medical masks.
Are they known to work?
The evidence behind the masks was recently reviewed and it turns out that not only were they never known to work, but that the evidence does not even rule out that they are harmful to you. Here is an excerpt from the report:
Wearing masks in the community probably makes little or no difference to the outcome of laboratory‐confirmed influenza/SARS‐CoV‐2 compared to not wearing masks (RR 1.01, 95% CI 0.72 to 1.42; 6 trials, 13,919 participants; moderate‐certainty evidence).
As you can see, not only does the point-estimate say that masks make you 1% more likely to contract COVID (RR = 1.01), but the evidence is consistent with masks making you up to 42% more likely to contract COVID (upper limit of 1.42).
Shall we ask Dr. Courtney if masks are “known to work?”
Remdesivir
In a review of the evidence behind the “standard-of-care” drug, Remdesivir, several kinds of outcomes were examined. Here is a recreated table of the findings:
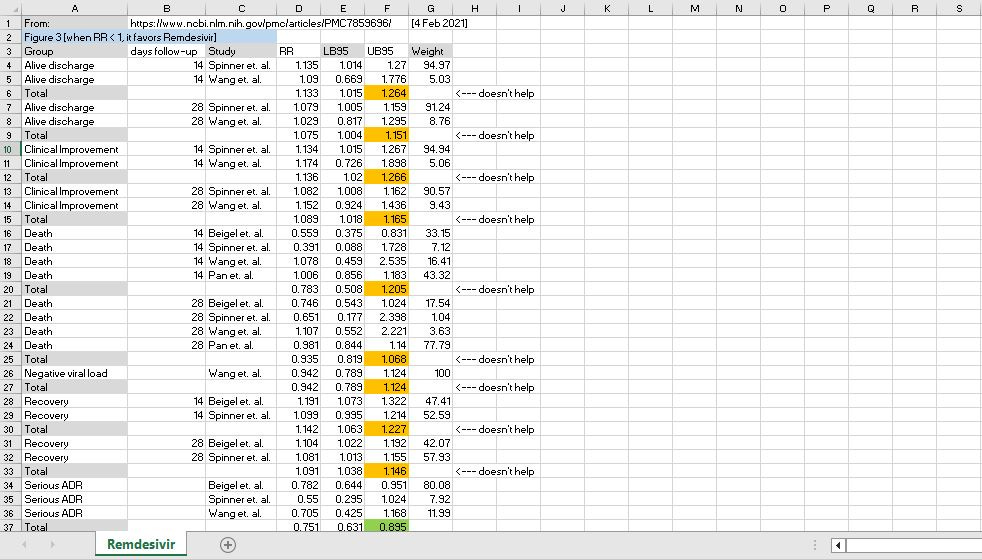
[click image to enlarge]
All of the summary findings, whether it was for being discharged alive at 14 or 28 days, experiencing clinical improvement in that same time, avoiding death in that same time, experiencing negative viral load, experiencing recovery — all of them — show evidence of Remdesivir not working.
Ivermectin
Yet a good analysis of the effects of ivermectin show that it reduced death by a minimum of 27% (upper bound of the risk interval). According to standards outlined above regarding when you “know” that a drug works for a condition, ivermectin is something that is known to work for COVID.
How do we know that ivermectin works?
Because the confidence interval around the benefit of ivermectin lies beyond a superiority margin of “20% benefit.” And you can’t say that about most of the “standard-of-care” interventions mandated or regimented during COVID.
This makes “expert witnesses” into hypocrites when they argue against upstanding physicians such as Dr. Nass.
They simultaneously support things that, under the highest standard of clinicial significance, are not known to work (e.g, masks, Remdesivir) — while, at the same time, criticizing prescriptions of things that are, under the highest standard of clinical significance, known to work (e.g., ivermectin).
Reference
[facemasks have no evidence of being beneficial for lab-confirmed COVID; even the point estimate doesn’t show benefit, let alone the limits of the confidence interval] — Physical interventions to interrupt or reduce the spread of respiratory viruses. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD006207.pub6/full
[no clinically-significant benefit of Remdesivir on any of the outomes examined] — Rezagholizadeh A, Khiali S, Sarbakhsh P, Entezari-Maleki T. Remdesivir for treatment of COVID-19; an updated systematic review and meta-analysis. Eur J Pharmacol. 2021 Apr 15;897:173926. doi: 10.1016/j.ejphar.2021.173926. Epub 2021 Feb 4. PMID: 33549577; PMCID: PMC7859696. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7859696/
[a 10% superiority margin is suggested, but the mean of effects deemed clinically-significant was 19.6%] — Gamad N, Shafiq N, Malhotra S. Meta-analysis of cardiovascular superiority trials published in the New England Journal of Medicine to elucidate the concept of superiority margin. Postgrad Med J. 2021 Apr;97(1146):227-233. doi: 10.1136/postgradmedj-2019-136569. Epub 2020 Mar 10. PMID: 32156742.
[the minimum survival benefit to be expected from ivermectin is a 27% improvement in survival] — Bryant A, Lawrie TA, Dowswell T, Fordham EJ, Mitchell S, Hill SR, Tham TC. Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines. Am J Ther. 2021 Jun 21;28(4):e434-e460. doi: 10.1097/MJT.0000000000001402. PMID: 34145166; PMCID: PMC8248252. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8248252/