
Expected Excess Mortality per Million
Flu vs. COVID. vs. Holocaust

The excess death per million expected with a bad year of flu is about 88 excess deaths per million. For perspective, the average kill rate of the Holocaust was 9100 per million — more than 100 times the excess death expected from bad flu.
Each year of the Holocaust was worth 103 flu seasons of death.
When groups of 16 nations get compared to each other, there will be some difference in the means of the groups, due to international variability. In one study, nations covering 57% of the entire world report excess death rate from flu.
Deliberately taking the lowest 16 values and forming a sample mean, and then contrasting it against that of the highest 16 values, it was discovered that when deaths are from natural causes such as acute respiratory disease, one sample mean for excess death can be almost 5 times as high as the other.
But that’s when deliberately choosing the extremes, so it represents a maximum expected multiple, or a MEM of 5.
While deaths by natural causes may only ever be found to have up to a 5-fold difference, deaths by artificial causes can reach much higher. The perfect example is the Holocaust cited above — worth 103 flu seasons of death, crammed into each and every year.
The Excel worksheet below has the top 16 nations (green) found in the OWID database reporting cumulative excess mortality per million (EM/M).
It also has the lowest 16 nations (yellow) reporting cumulative excess mortality per million (EM/M).
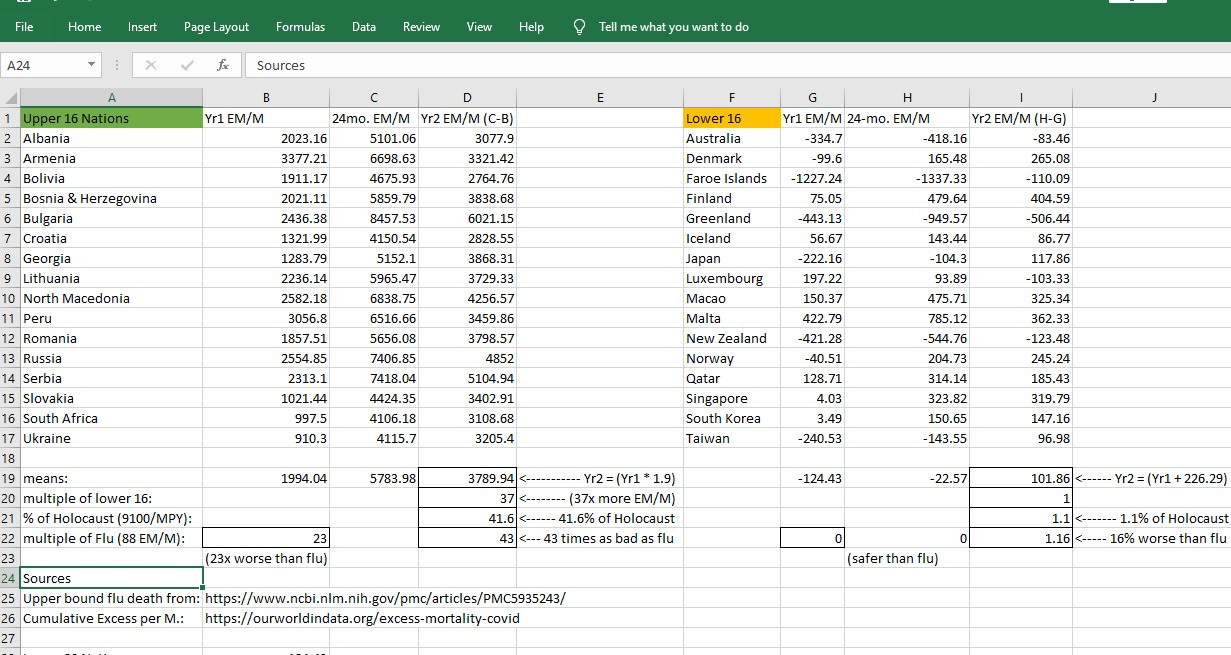
The notes at bottom describe how, in the upper 16 nations, excess death in 2021 was 90% worse than 2020 — indicating that vaccines are harmful. Compared to the lowest 16 nations, the top 16 had a mean which was 37 times as high.
But a 37-fold increase in mean excess death rates is far beyond the maximum expectation of a 5-fold increase (and no higher than that). This indicates that deaths in 2021 were not from natural causes like infectious diseases, etc.
The upper nations in 2021 saw excess death rates 43 times worse than flu, reaching about 41.6% of Holocaust-level death rates. The lower 16 nations didn’t have any average excess death from COVID — at least not until COVID vaccines became available.
After vaccines were made available, the excess death rate rose.
Reference
[Cumulative Excess Death per million] — OWID data. Available: https://ourworldindata.org/excess-mortality-covid
[2017/18 Weekly P&I deaths] — CDC “FluView” online tool. Available: https://gis.cdc.gov/grasp/fluview/mortality.html
[Annualized 0.91% kill rate of Holocaust (Germany + Occupied Europe)] — DEMOCIDE: NAZI GENOCIDE AND MASS MURDER. 20,946,000 Victims: Nazi Germany 1933 To 1945. By R.J. Rummel. Available: https://hawaii.edu/powerkills/NAZIS.CHAP1.HTM
[As of 19 Jan 2021, from 52,000 COVID infections with Alpha (SGTF) variant, there were 104 deaths (observed Alpha IFR=0.2%)] — UK Technical Briefing #5 (PDF file). Available general: https://www.gov.uk/government/publications/investigation-of-novel-sars-cov-2-variant-variant-of-concern-20201201
Available specific page: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/959426/Variant_of_Concern_VOC_202012_01_Technical_Briefing_5.pdf
[Table 3: In almost 700,000 cases confirmed by sequencing, Delta was 42% as lethal as Alpha (imputed Delta IFR=0.08%)] — UK Technical Briefing #25. Available general: https://www.gov.uk/government/publications/investigation-of-sars-cov-2-variants-technical-briefings
Available specific page: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1025827/Technical_Briefing_25.pdf
[From 1.5 million confirmed cases, Omicron is (at most) 41% as lethal as Delta (IFR = 0.034%)] — Nyberg T, Ferguson NM, Nash SG, Webster HH, Flaxman S, Andrews N, Hinsley W, Bernal JL, Kall M, Bhatt S, Blomquist P, Zaidi A, Volz E, Aziz NA, Harman K, Funk S, Abbott S; COVID-19 Genomics UK (COG-UK) consortium, Hope R, Charlett A, Chand M, Ghani AC, Seaman SR, Dabrera G, De Angelis D, Presanis AM, Thelwall S. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022 Mar 16:S0140-6736(22)00462-7. doi: 10.1016/S0140-6736(22)00462-7. Epub ahead of print. PMID: 35305296; PMCID: PMC8926413. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8926413/
[top 16 nations had mean flu excess death rates 4.8 times higher than the mean of the bottom 16 nations (age 65-74 bracket)] — Iuliano AD, Roguski KM, Chang HH, Muscatello DJ, Palekar R, Tempia S, Cohen C, Gran JM, Schanzer D, Cowling BJ, Wu P, Kyncl J, Ang LW, Park M, Redlberger-Fritz M, Yu H, Espenhain L, Krishnan A, Emukule G, van Asten L, Pereira da Silva S, Aungkulanon S, Buchholz U, Widdowson MA, Bresee JS; Global Seasonal Influenza-associated Mortality Collaborator Network. Estimates of global seasonal influenza-associated respiratory mortality: a modelling study. Lancet. 2018 Mar 31;391(10127):1285-1300. doi: 10.1016/S0140-6736(17)33293-2. Epub 2017 Dec 14. Erratum in: Lancet. 2018 Jan 19;: PMID: 29248255; PMCID: PMC5935243. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5935243/
Pull-quote:
“EMR[excess mortality rate]-contributing countries represented 57% of the global population. The estimated mean annual influenza-associated respiratory EMR ranged from ... 2·9 to 44·0 per 100 000 individuals for people aged between 65 and 74 years ... . We estimated that 291 243–645 832 seasonal influenza-associated respiratory deaths (4·0–8·8 per 100 000 individuals) occur annually.”