

Flu vs. COVID vs. "COVID shots"
Flu vs. COVID vs. "COVID shots"
Head-to-Head Risk Comparison

Intro to Safety Signals: Meaning and Use
A safety signal is a sign of harm from a new treatment. In pharmacovigilance studies, safety signals are followed-up on if the potential additional risk is meaningful, and if the relationship of cause to effect can be adequately ascertained.
An example of a safety signal which was deemed too weak to follow-up on is the association of pancreatic cancer with the use of the arthritis medication, tofacitinib (tofa-citi-nib), made by Pfizer.
The additional risk was meaningful, but the relationship of cause to effect was too spurious to invest resources to follow-up on and precisely measure if there is indeed added harm from the drug.
The meaningful risk was a doubling (or, most conservatively, a tripling) of baseline pancreatic cancer rates. The baseline rate is around 60 to 90 annual cancer cases per million person-years.
Five-year survival is poor for pancreatic cancer, as low as just 10%, so the baseline death rate might be 54 to 81 annual cancer deaths per million person-years.
The pooled case rate for psoriasis patients receiving the drug was 700 cases per million person-years, but the lower bound of the CI95 interval was 200 cases per million person-years.
At only 10% survival, that is equivalent to 180 annual deaths per million person-years.
Because an extra 110 annual cases (200 - 90) of pancreatic cancer per million person-years is clinically meaningful — it may cause an extra 101 (180 - 81) deaths per million person-years, which is high enough for “action” — a sensitivity analysis was performed and pancreatic cancer cases found within 6 months of initiation of treatment were removed, dropping the CI95 lower bound to 100 cases per million.
If males get 90 annual pancreatic cancer cases per million, and the lower bound of the estimate is just 100 annual cases per million, then ruling out a difference requires tens of thousands of person-years of observation — because the baseline rate is already so low.
They ended up not looking into the connection, based on the resources and data required to rule out a doubling of pancreatic cancer incidence from taking the drug
But the take-away message is that, if a treatment DID double or triple the baseline rate — i.e., if it caused an extra ~100 annual deaths per million — then it’d lead to “action” because that much extra death is “too much” extra harm, at least as measured against the benefit of treating arthritis.
Use of Fermi Questions to uncover Perspective and Proportionality
Put into hard numbers using Fermi Questions (questions all answerable by rough approximations), at most 4% of a nation has the kind of arthritis required for this drug to be used.
In a nation of 330 million, that’s 13 million “possible” recipients of tofacitinib. But it isn’t a first-line treatment, and maybe only 5 million would ever need more than first-line treatment. But tofacitinib is only one of several second-line treatments. Of those 5 million seeking second-line treatment, only as little as 1 million would get tofacitinib.
If the drug adds an extra 100 deaths per million, and a highly-plausible total number of patients receiving the drug is 1 million — then the added death from the drug would sum up to 100 added deaths per year.
This much extra death per year — just one hundred extra people dying — is enough harm to get a drug either pulled from the market, or to AT LEAST get a bold warning added to the label.
RECAP: Arthritis drugs are compounds which should be so safe that they would not be expected to kill 100 people per year (100 annual deaths is “too much”).
Dr. Peter McCullough has been saying that just 50 unexplained deaths got vaccines pulled, and vaccines are usually for diseases more serious than arthritis.
And remember, this was from the Pfizer study itself. It was they who, possibly inadvertantly, defined what “too much” looks like — and then they found out if they could prove or disprove (rule out) the connection.
The entire Pfizer study is an implicit admisson that 100 extra annual deaths is too much extra death (i.e., that arthritis drugs shouldn’t be made, or should at least have bold warnings, if they are expected to kill an extra 100 people each year).
COVID vs. A Bad Year of Flu
A bad year of flu was the season from Fall of 2014 to Spring of 2015. The CDC reported just over 50,000 flu deaths for that season, and one of the worst statistics was the death rate of those hospitalized for flu, which was almost 9% of the hospitalized ending up dying.
CDC estimates symptomatic cases, but only around 84% of all flu infections are symptomatic (16% never get symptoms). Adjusting the CDC numbers reveals the underlying flu “infection rate” which is, by definition, higher than the symptomatic case rate. Here is a breakdown in Excel:
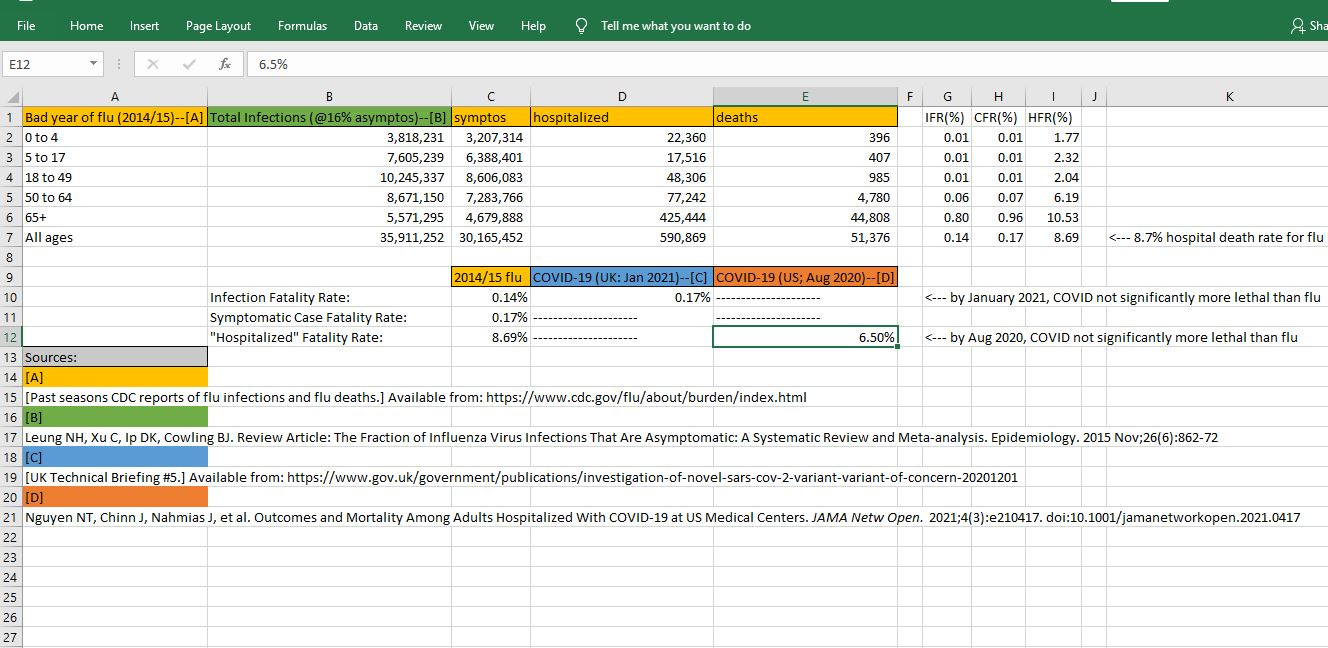
Notice how the infection fatality rate (IFR) of COVID in the UK in January of 2021 (cell D10) was higher than the IFR for a bad year of flu (cell C10) — but that it was just 21% higher, so that it is unlikely that it would be a significant finding.
By January 2021, COVID fatality was “trending higher” than a bad year of flu, but from a statistics perspective, COVID fatality would be interpeted as being similar to a bad year of flu.
By August of 2020, the combination of reduced susceptibility out of those with low natural immunity to COVID, along with improved COVID treatments, had made it so that the average hospital COVID death rate among 555 US medical centers was just 6.5%.
On just the metric of “How much of those hospitalized for this disease will die?” — COVID had become “safer” than a bad year of flu.
Given the vast and detailed data in the UK, by January 2021, properly performed statistical tests would no longer find COVID as being statistically more deadly than flu — at least when looking at all of the COVID variants which came after the Alpha variant (Delta variant included).
Back to the Safety Signal
The VAERS data indicates really high harm from COVID shots, but government officials attempt to dismiss the “safety signal” by saying that it is just reporting bias/notorioty bias (if a risk is “in the news” more people report it).
A safety signal regarding sudden cardiac arrest (SCA) and sudden cardiac death (SCD) has been found to coincide with the COVID shots, but if the passive surveillance signal that you get from the VAERS data is dismissed, then officials won’t respond appropriately to it and follow-up.
Statistical evidence from just one week of just one type of professional athlete (FIFA players) is already strong enough, however. And, importantly, it cannot be dismissed out of hand, unless you hypothesize something really very crazy: athletes “faking” their own deaths.
Here is an alarming week of deaths in FIFA at the end of December 2021, after players had received COVID shots:
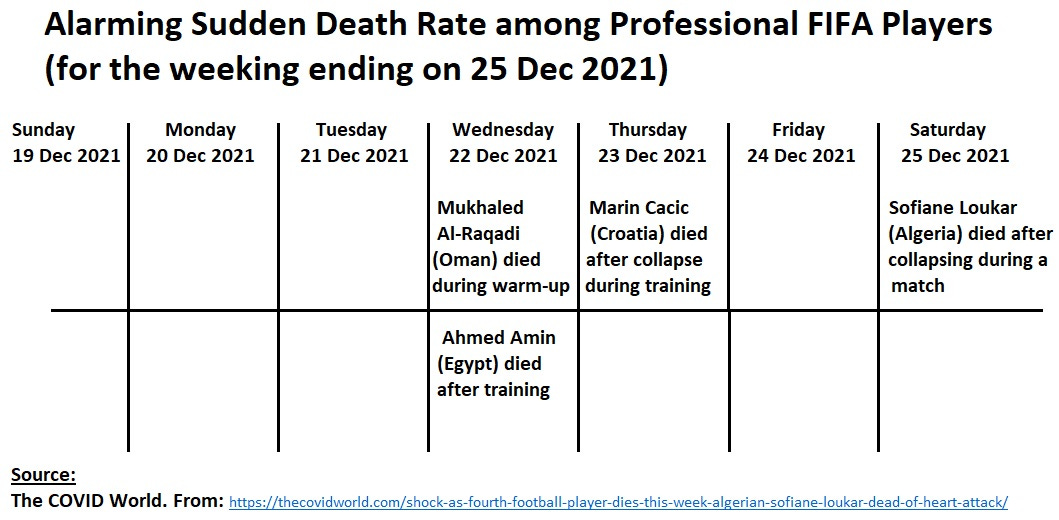
The sudden death count for this week is 4 and to give it perspective requires that one know about the baseline expected death count for the entire 10-month season: 4.8 expected sudden deaths.
This peak weekly sudden death rate is 36 times the expected average rate.
Here is an Excel spreadsheet showing how the baseline rate and count were derived, and also showing the statistical probability of a week with 4 deaths and how it is clearly — by all scientific standards — a safety signal of harm:
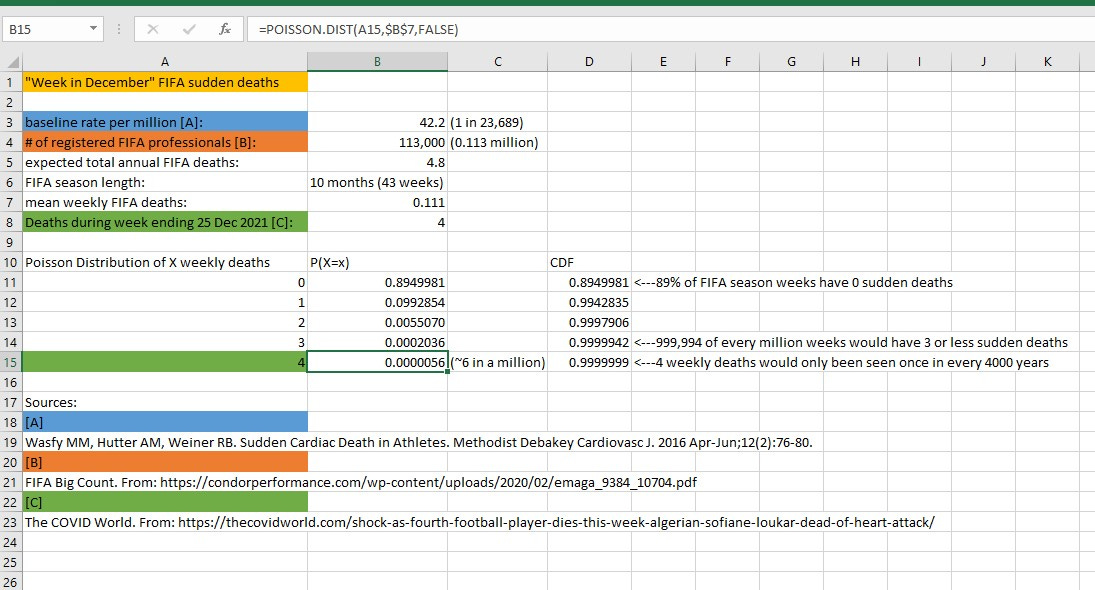
The baseline chance of getting 4 FIFA sudden deaths to occur within one week is something so rare it would only happen randomly only 6 times in a million. Put into persective, that sudden death count for that week is something you’d only ever see by chance once in every 4000 years.
Caution: If you are seeing death outcomes that are so rare that they’d only occur just once in every 4000 years, then you have a safety signal on your hands. Whether it is followed-up or not is another matter. But the existence of the signal is a scientific fact.
Synopsis
By January of 2021, the lethality of the circulating variants of COVID was already statistically indistinguishable from a bad year of flu. Evidence even as early as August 2020 revealed that the “COVID scare” was already being overplayed, because less than 7% of COVID-hospitalized patients were dying (something similar to flu hospital deaths rates).
Once the Delta variant predominated by the end of Summer of 2021, only flu-like death rates would be expected to occur — and only COVID treatments which were not more dangerous than flu treatments should remain in use.
If COVID shots are more dangerous than flu shots, then they should not be used.
That’s because COVID is no longer statistically more lethal than flu, and it hasn’t been more lethal than flu since at least end of summer 2021, and possibly for more than a year now.
Yet evidence from just one week of professional athletes experiencing sudden deaths is already indicative that COVID shots are much more dangerous than flu shots — perhaps by an order of magnitude.
It makes no sense to take a treatment which is up to 10 times more dangerous than usual treatments, for an acute respiratory disease which is not (statistically) more dangerous than usual acute respiratory disease.
It violates the purpose behind forming a risk:benefit ratio in the first place (i.e., to do the most good, but only if it can be done with the least harm). First, do no harm.
Reference
[Example of review of Safety Signal] Safety signal detection and evaluation in clinical development programs: A case study of tofacitinib. Gorana Dasic, Thomas Jones, Vera Frajzyngier, Ricardo Rojo, Ann Madsen, Hernan Valdez.
First published: 15 December 2017
https://doi.org/10.1002/prp2.371
Funding information: This work was funded by Pfizer Inc.
[Past seasons CDC reports of flu infections and flu deaths.] Available from: https://www.cdc.gov/flu/about/burden/index.html
[Fraction of flu infections with symptoms] Leung NH, Xu C, Ip DK, Cowling BJ. Review Article: The Fraction of Influenza Virus Infections That Are Asymptomatic: A Systematic Review and Meta-analysis.
[COVID IFR from UK Technical Briefing #5.] Available from: https://www.gov.uk/government/publications/investigation-of-novel-sars-cov-2-variant-variant-of-concern-20201201
[August 2020 hospital death rate for COVID] Nguyen NT, Chinn J, Nahmias J, et al. Outcomes and Mortality Among Adults Hospitalized With COVID-19 at US Medical Centers. JAMA Netw Open.
[4 sudden deaths in a single week in FIFA] The COVID World. From: https://thecovidworld.com/shock-as-fourth-football-player-dies-this-week-algerian-sofiane-loukar-dead-of-heart-attack/
[Total number of professional FIFA players] FIFA Big Count. From: https://condorperformance.com/wp-content/uploads/2020/02/emaga_9384_10704.pdf
[Baseline sudden death in athletes] Wasfy MM, Hutter AM, Weiner RB. Sudden Cardiac Death in Athletes. Methodist Debakey Cardiovasc J. 2016 Apr-Jun;12(2):76-80.