
Implied Cost-Effectiveness shows COVID Jabs fail
Using CDC data on prevented hospitalizations to infer prevented deaths

If a medicine or a medical intervention can save a year of live for twice your personal income or less, then it is considered cost effective. Because median personal income was approximately $35,000 in 2021, cost-effective medicines for at least half of the USA would save a life-year for $70,000 or less.
A review of vaccines shows that most (60%) were able to save a quality-adjusted life-year (QALY) for under $50,000 in constant 2016 dollars. But COVID jabs are another story.
CDC data on the number of doses required to prevent a hospitalization show that it compares poorly to typical vaccines.
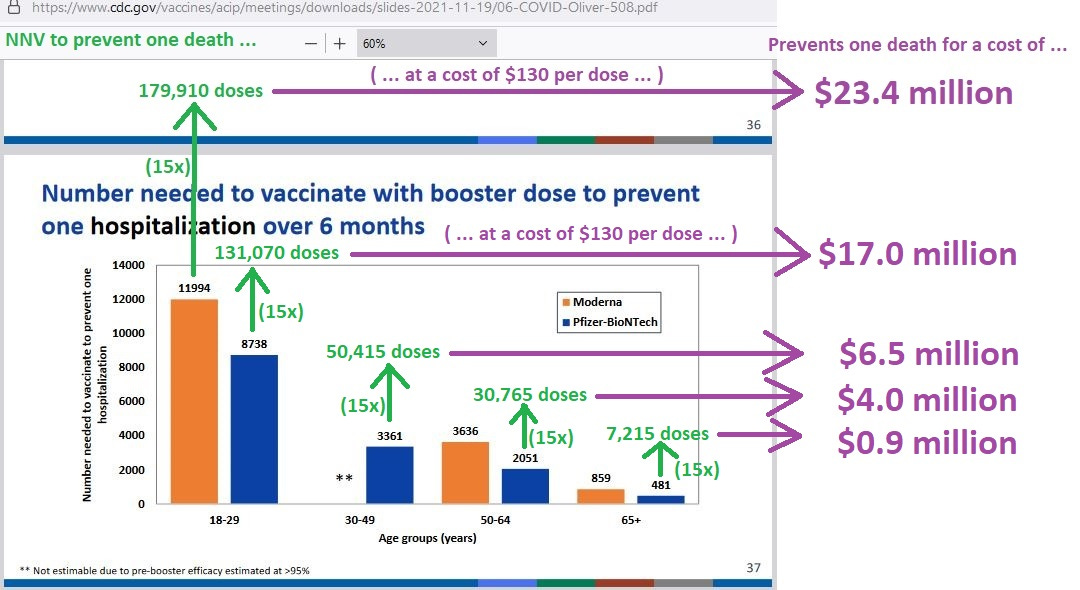
Using the estimated hospital death rate arrived at under the original strain of COVID — 6.5% of the hospitalized died (which is approximately 1 in 15) — you can get the number of doses required to prevent one single COVID death, and then you can get the cost of preventing that single death.
Because the prevailing variant of COVID (Omicron) is less deadly, and CDC data used a more virulent COVID variant, the higher of two estimates of COVID jab prices is used. The low estimate is $110, but the high estimate of $130 per dose is used, to balance out the lower virulence of Omicron.
Where are the numbers, you ask? Here are the numbers:
Because being “cost-effective” requires saving a life-year for $70,000 or less (at least for 50% of the US population), you can estimate the number of years that you must expect to live to see if the COVID jab is a cost-effective medical intervention.
In those below age 30, Moderna boosters would cost $23.4 million per whole life saved — meaning that those in that age group would need to live for another 335 years on average, to make the COVID jab cost-effective on a “per-life-year-saved” standard.
The other 4 estimates are for Pfizer, but they are not much better. Those under age 30 still need to live for another 244 years on average, to make the booster “cost-effective.” Even those under age 50 still need to live for another 94 years on average, in order for the COVID jab to be considered “cost-effective.”
Reference
[Hospitalized COVID patients followed in 555 US Medical Centers: hospital death rate down to 6.5% by August 2020] — Nguyen NT, Chinn J, Nahmias J, Yuen S, Kirby KA, Hohmann S, Amin A. Outcomes and Mortality Among Adults Hospitalized With COVID-19 at US Medical Centers. JAMA Netw Open. 2021 Mar 1;4(3):e210417. doi: 10.1001/jamanetworkopen.2021.0417. PMID: 33666657; PMCID: PMC8547263. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8547263/
[Gaining a life-year at a cost equal to or less than twice your income is an appropriate cut-off for “cost-effectiveness”] — Garber AM, Phelps CE. Economic foundations of cost-effectiveness analysis. J Health Econ. 1997 Feb;16(1):1-31. doi: 10.1016/s0167-6296(96)00506-1. PMID: 10167341. https://pubmed.ncbi.nlm.nih.gov/10167341/
[Median household income (2021)] — U.S. Census Bureau, Median Household Income in the United States [MEHOINUSA646N], retrieved from FRED, Federal Reserve Bank of St. Louis; https://fred.stlouisfed.org/series/MEHOINUSA646N
[Employment-age persons] — U.S. Bureau of Labor Statistics, Population Level [CNP16OV], retrieved from FRED, Federal Reserve Bank of St. Louis; https://fred.stlouisfed.org/series/CNP16OV
[Number of US households] — U.S. Census Bureau, Total Households [TTLHH], retrieved from FRED, Federal Reserve Bank of St. Louis; https://fred.stlouisfed.org/series/TTLHH
[Most (60% of) vaccines save a life-year for less than $50,000 in constant 2016 dollars] — Leidner AJ, Murthy N, Chesson HW, Biggerstaff M, Stoecker C, Harris AM, Acosta A, Dooling K, Bridges CB. Cost-effectiveness of adult vaccinations: A systematic review. Vaccine. 2019 Jan 7;37(2):226-234. doi: 10.1016/j.vaccine.2018.11.056. Epub 2018 Dec 4. PMID: 30527660; PMCID: PMC6545890. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6545890/