


Jab counterproductivity to age 35 (myocarditis)
Post #533

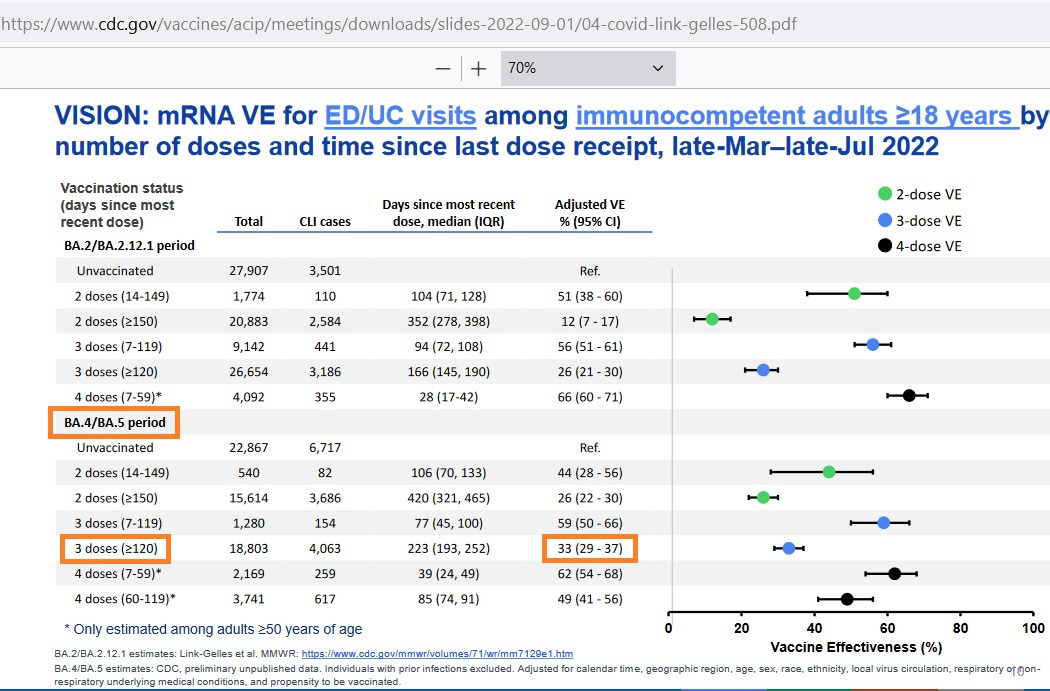
The effectiveness of booster shots wanes over time and is also age-dependent. If you are age 18 and over, booster shot effectiveness after 120 days is only 33%:
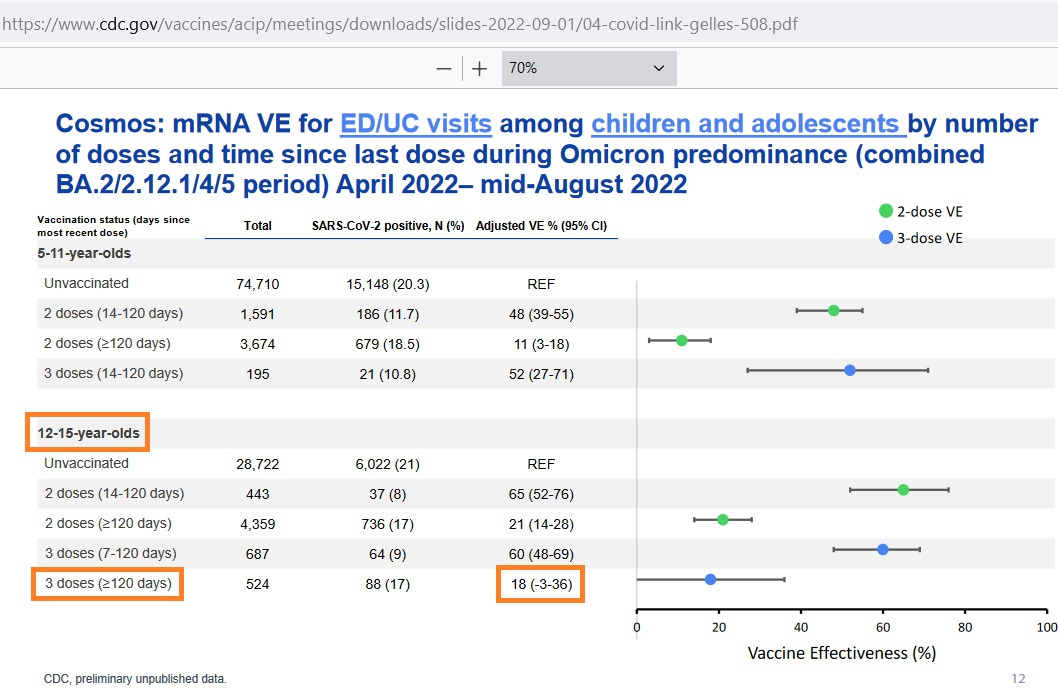
But if you are under age 16, the effectiveness of the booster shot is even lower:
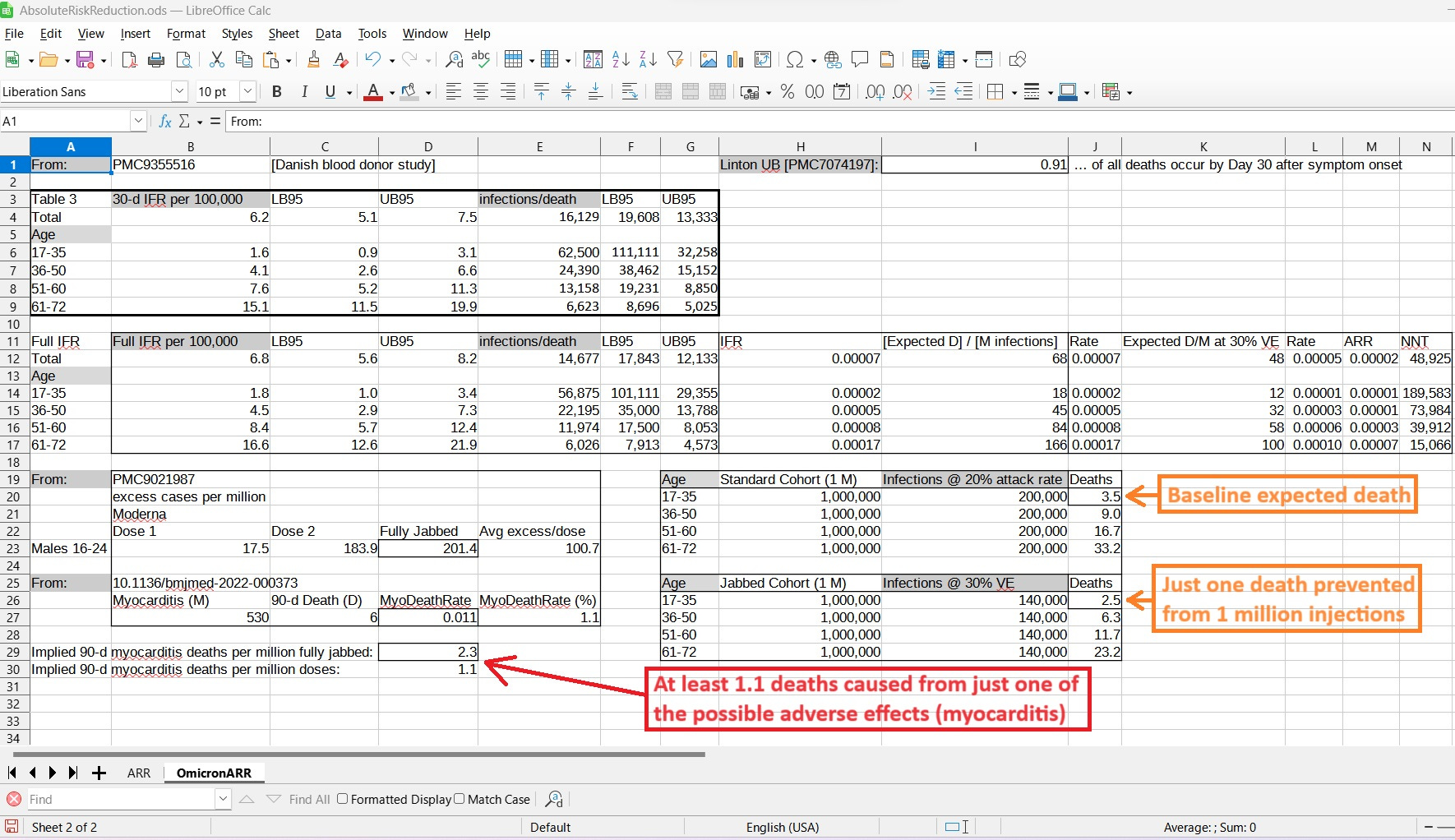
For the purpose of evaluating if myocarditis deaths outweigh Omicron deaths prevented by booster shots, here is an analysis showing the assumptions and the results:
[click to enlarge]
The top left shows results of a Danish study involving blood donors, and the Omicron infection fatality rate for those from age 17 to 35 was just 1.6 per 100,000 infections (16 per million). To give perspective on that, a 6-season average death from flu for those of age 18-49 was 14.8 per 100,000 flu infections (148 per million).
For those under age 36, flu is almost 10 times worse than Omicron variant COVID.
At middle left is the result of 23 million Nordic people tracked over time. Among males of age 16 to 24, Moderna doses led to 17.5 (dose 1) and 183.9 (dose 2) excess myocarditis cases per million. Taken together, that was 201.4 excess cases per million fully-jabbed Moderna recipients.
At bottom left is the 90-day lethality of myocarditis cases associated with COVID jabs — also using the Nordic sample. The 90-day fatality rate was 1.1%.
At middle-bottom are two standard cohorts of one million men of age 17-35. The top cohort is the baseline, where 20% are assumed to be infected each period, and 3.5 of those million people are expected to die from COVID.
The bottom of the two cohorts assumes all one million of the men get jabbed, and they end up with 30% less COVID (a crude average of adult VE and the VE for 12-15 year-olds), and they get one less death.
But if you jab a million men, Nordic data indicate that you’ll cause somewhere from 1.1 to 2.3 deaths from myocarditis.
This harm:benefit scenario only takes into account one adverse effect from COVID shots (myocarditis) and it is already “negative” for males under age 36. What happens when we add in the other harms from the shots?
Reference
[kids get 18% VE from boosters by Day 120; adults get 33%] — CDC Presentation. Slide 14. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2022-09-01/04-covid-link-gelles-508.pdf
[age 18-49 flu IFR (assuming 16% asymptomatics) for 2012-2019 flu seasons, with 2017/18 omitted] — CDC. Burden of Flu. https://www.cdc.gov/flu/about/burden/index.html
[6 of 530 (1.1%) myocarditis cases died] — Husby A, Gulseth HL, Hovi P, Hansen JV, Pihlström N, Gunnes N, Härkänen T, Dahl J, Karlstad Ø, Heliö T, Køber L, Ljung R, Hviid A. Clinical outcomes of myocarditis after SARS-CoV-2 mRNA vaccination in four Nordic countries: population based cohort study. BMJ Med. 2023 Feb 1;2(1):e000373. doi: 10.1136/bmjmed-2022-000373. PMID: 36936260; PMCID: PMC9978676. https://pubmed.ncbi.nlm.nih.gov/36936260/
[over 200 excess myocarditis cases per million men fully dosed with Moderna] — Karlstad Ø, Hovi P, Husby A, Härkänen T, Selmer RM, Pihlström N, Hansen JV, Nohynek H, Gunnes N, Sundström A, Wohlfahrt J, Nieminen TA, Grünewald M, Gulseth HL, Hviid A, Ljung R. SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents. JAMA Cardiol. 2022 Jun 1;7(6):600-612. doi: 10.1001/jamacardio.2022.0583. PMID: 35442390; PMCID: PMC9021987. https://pubmed.ncbi.nlm.nih.gov/35442390/
[very low Omicron IFR for those under age 36] — Erikstrup C, Laksafoss AD, Gladov J, Kaspersen KA, Mikkelsen S, Hindhede L, Boldsen JK, Jørgensen SW, Ethelberg S, Holm DK, Bruun MT, Nissen J, Schwinn M, Brodersen T, Mikkelsen C, Sækmose SG, Sørensen E, Harritshøj LH, Aagaard B, Dinh KM, Busch MP, Jørgensen CS, Krause TG, Ullum H, Ostrowski SR, Espenhain L, Pedersen OBV. Seroprevalence and infection fatality rate of the SARS-CoV-2 Omicron variant in Denmark: A nationwide serosurveillance study. Lancet Reg Health Eur. 2022 Oct;21:100479. doi: 10.1016/j.lanepe.2022.100479. Epub 2022 Aug 5. PMID: 35959415; PMCID: PMC9355516. https://pubmed.ncbi.nlm.nih.gov/35959415/