

It can be difficult to find out just how bad things are for a medical product when looking at published research. That’s because there are perverse incentivizes to magnify benefits and minimize harms, in order to maintain public enthusiasm for the product and to prevent any hesitancy. But if you search hard, you can find gems.
When Canadian researchers looked for myocarditis after COVID shots, they found 14x what was expected (for both sexes and all ages, combined):

[click to enlarge]
The expected yearly rate of myocarditis runs from 1-10 per 100,000 person-years, meaning that — viewed weekly — you can expect to find anywhere from 1/52 up to 10/52 (or from 0.02 to 0.2) cases of myocarditis per 100,000 person-weeks:

But if the highest rate that you would ever expect is 0.2 cases per 100,000 person-weeks, then any numbers above 0.2 represent “excess myocarditis” (myocarditis attributable to some environmental cause). For the 3rd dose of Pfizer, young males in the first week had 7.01 cases per 100,000 — at least 35x the highest expected baseline rate:

[click to enlarge]
Because the researchers compared these cases to those found in 2019 — which for this group were much lower than the maximum expected rate of 0.2 weekly cases per 100,000 — they came up with an observed-to-expected (OE) ratio even higher than 35x (they came up with 140x):

[click to enlarge]
Another way to look at this is to compare myocarditis rates across doses, and even maybe across countries (though this second method is problematic, due to national differences). Look at these weekly reports per million after Pfizer shots in males:

If the US rate for age 16-17 males is reflected by the one found after Dose 1 (7.3 weekly cases per million; equivalent to 0.73 weekly cases per 100,000) — which is a very generous assumption (because 0.2 weekly cases per 100,000 is as high as you would ever expect) — how do we explain the Dose 2 rate of 105.9 weekly cases per million?
Also note how it was that, for males of age 12-17 in Hong Kong, the rate after Dose 2 was 150 times the highest rate that you would ever expect (0.2 weekly cases per 100,000 = 2 cases per million person-weeks, but Hong Kong had 311 cases in the first week after Dose 2).
Check out these weekly rates per million for males taking Moderna:
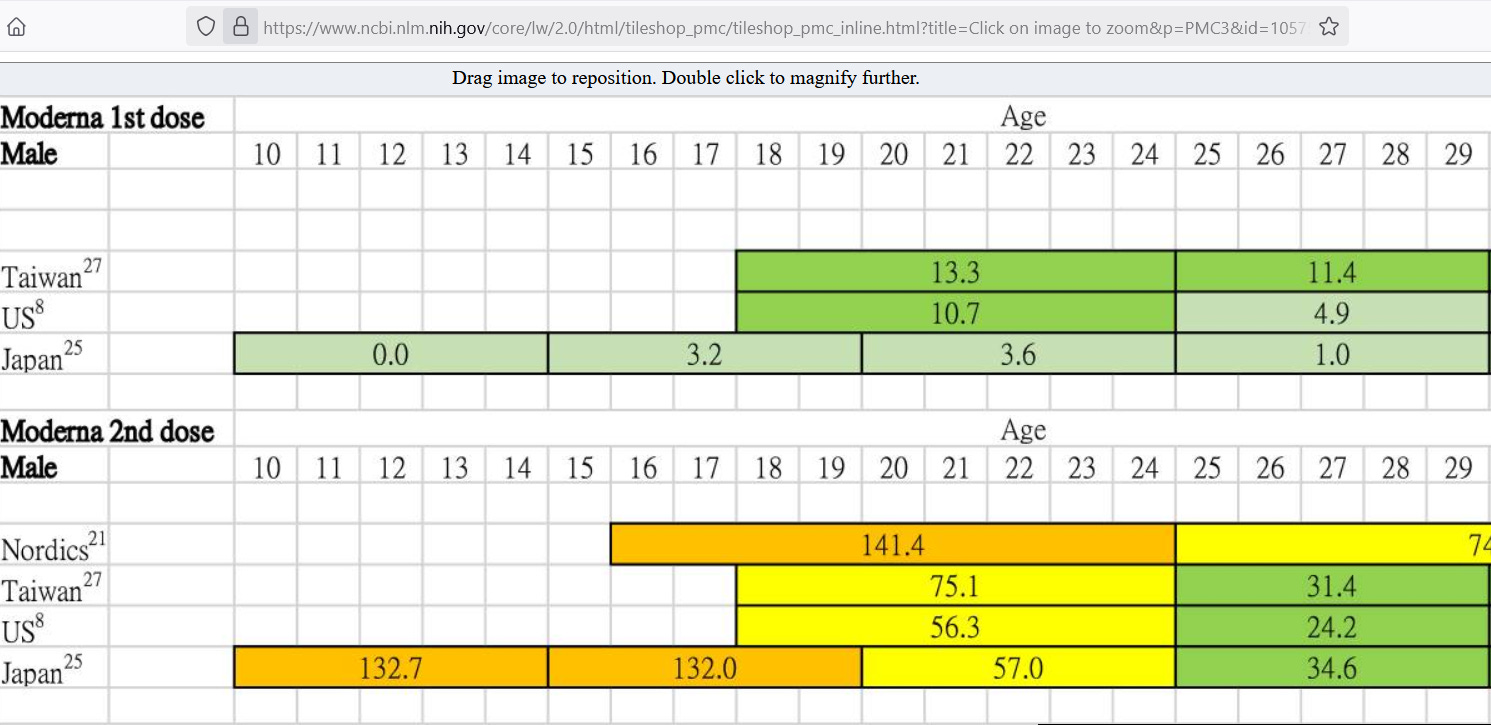
For males in Japan of age 15-19, the first dose of Moderna led to 3.2 weekly cases per million. If that rate is assumed as the baseline myocarditis rate for this group, then how do we explain the weekly rate after Dose 2 (132 weekly cases per million)? The weekly rate after Dose 2 for them was 41x the weekly rate after Dose 1 for them.
But medical products should not be making you at least 35-41 times more likely to experience a serious adverse event, such as myocarditis. Myocarditis can scar the heart for life, reducing your chances of having a full life. In the short-to-medium term, between 1% and 7% of myocarditis cases are fatal:

The evidence suggests that COVID shots should not have been allowed to have remained on the market for children, especially for males. Being at least 35 times more likely to experience a condition that is at least 1% fatal is just too much risk to expose our children to, given their very low baseline risk of harm from COVID.
Reference
[at least 35x the expected rate of myocarditis for young Canadian males] — https://www.cmaj.ca/content/194/45/e1529
[the highest expected myocarditis rate is 10 per 100,000 person-years (weekly = 0.2 per 100,000 person-weeks)] — https://www.nature.com/articles/s41569-021-00662-w
[weekly myocarditis rates per million doses] — Lin YC, Chang CH, Su WJ, Yang CH, Wang JT. Risk of Coronavirus Disease 2019 Messenger RNA Vaccination-Associated Myocarditis and Pericarditis - A Systematic Review of Population-Based Data. Risk Manag Healthc Policy. 2023 Oct 9;16:2085-2099. doi: 10.2147/RMHP.S422372. PMID: 37841076; PMCID: PMC10575036. https://pmc.ncbi.nlm.nih.gov/articles/PMC10575036/
[myocarditis is up to 7% fatal] — https://heart.bmj.com/content/early/2025/04/17/heartjnl-2024-325523