

A healthy vaccinee bias arises because the people who get vaccinated are typically healthier than those who refrain. Because they die less (because they were healthier to begin with), we have to correct vaccine statistics to account for the different expectations. Tracy Beth Hoeg presented on some of the magnitudes of correction:
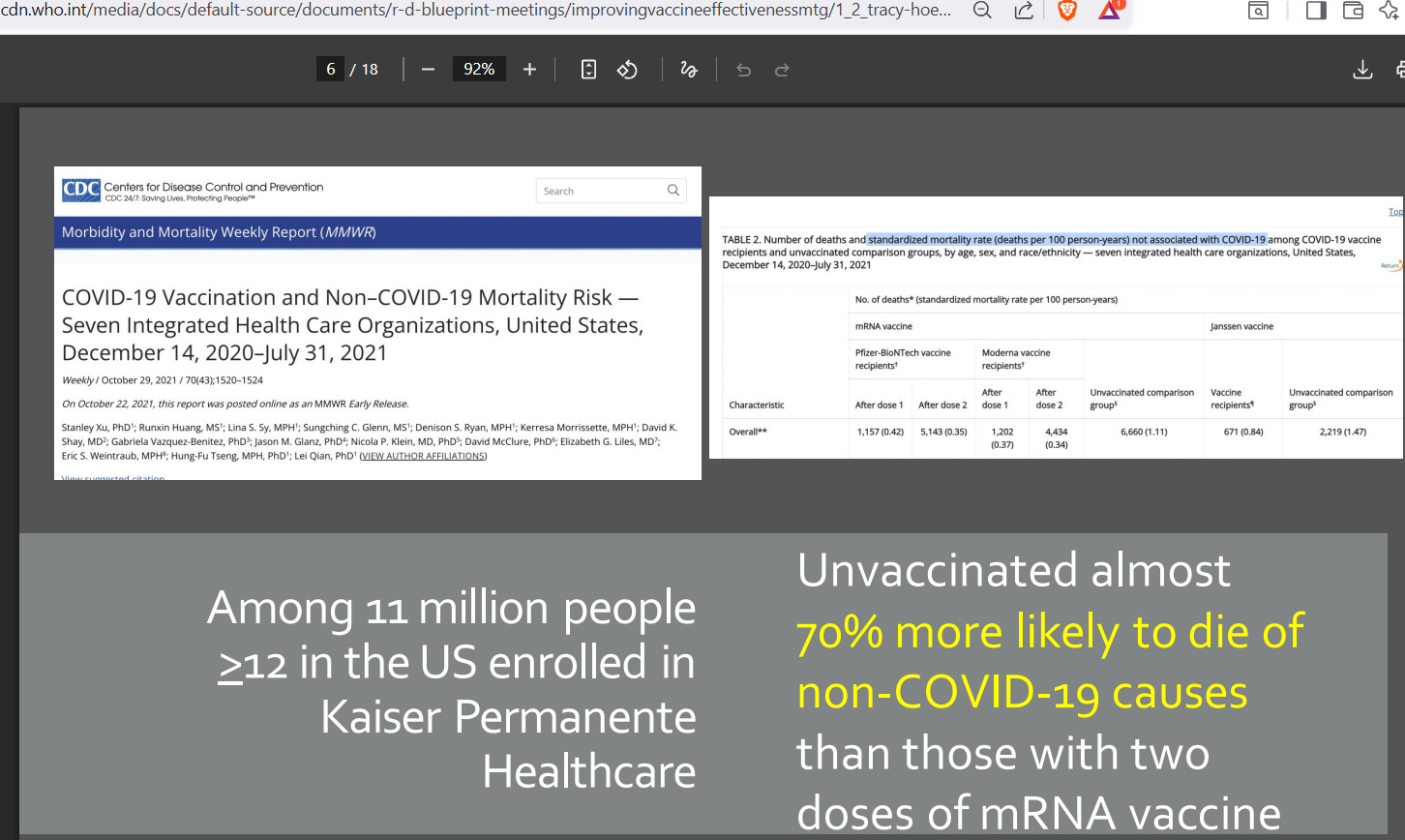
If those who are unvaccinated are 70% more likely to die from non-COVID causes, then it indicates that the healthy vaccinee bias is 41% — i.e, people choosing to get vaccinated were so much healthier that they die at only 59% of the rate of the unvaccinated group.
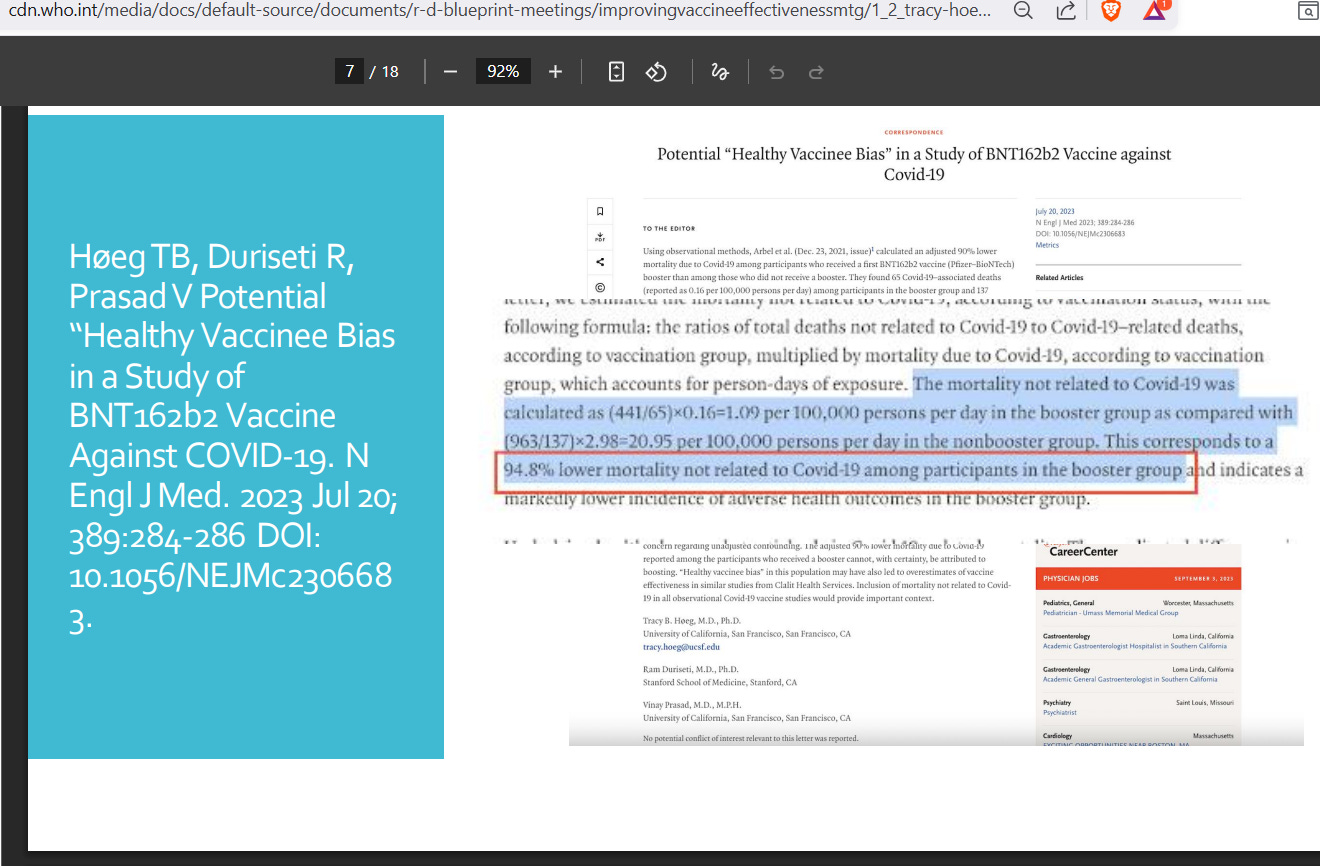
If those who are vaccinated have a 94.8% lower chance to die from non-COVID causes, then it indicates that the healthy vaccinee bias is ~95% — i.e, people choosing to get vaccinated were so much healthier, that they die at only 51% of the rate of the unvaccinated group.
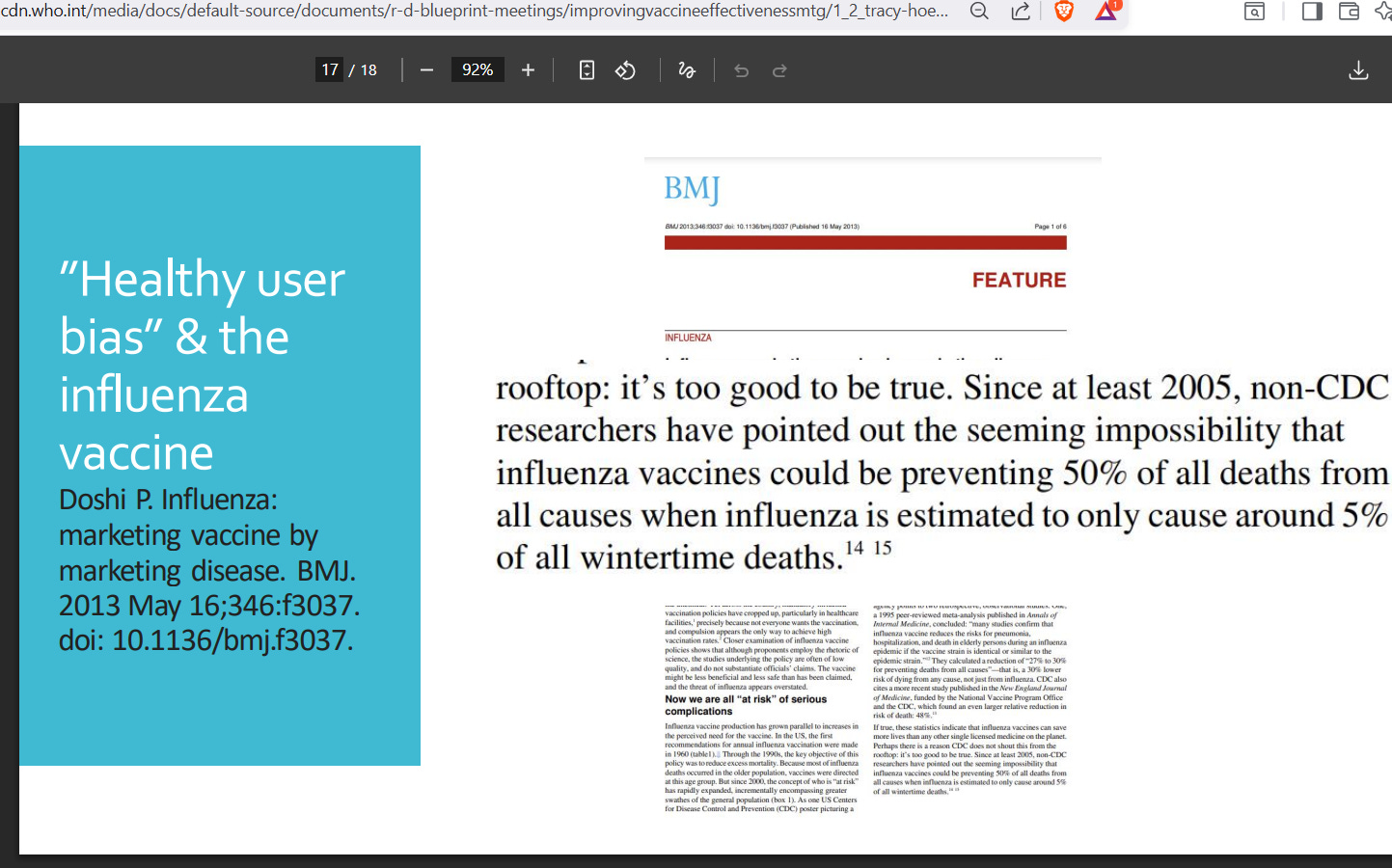
If 45% of all death reduction cannot be explained by avoiding flu, then that means that the healthy vaccinee bias is 45% — i.e, people choosing to get vaccinated were so much healthier that they die at only 55% of the rate of the unvaccinated group. These estimates indicate a magnitude of at least 40% on healthy vaccinee bias.
But what is a good minimum value of healthy vaccinee bias?
A good minimum value for healthy vaccinee bias
After finding a value that serves as a good minimum, then any future data set purporting to show vaccine benefit or harm could be corrected by that minimum estimate of bias. A study in Qatar helps to uncover a minimum value that should be used on a first-pass (i.e., without any questions) for health vaccinee bias:
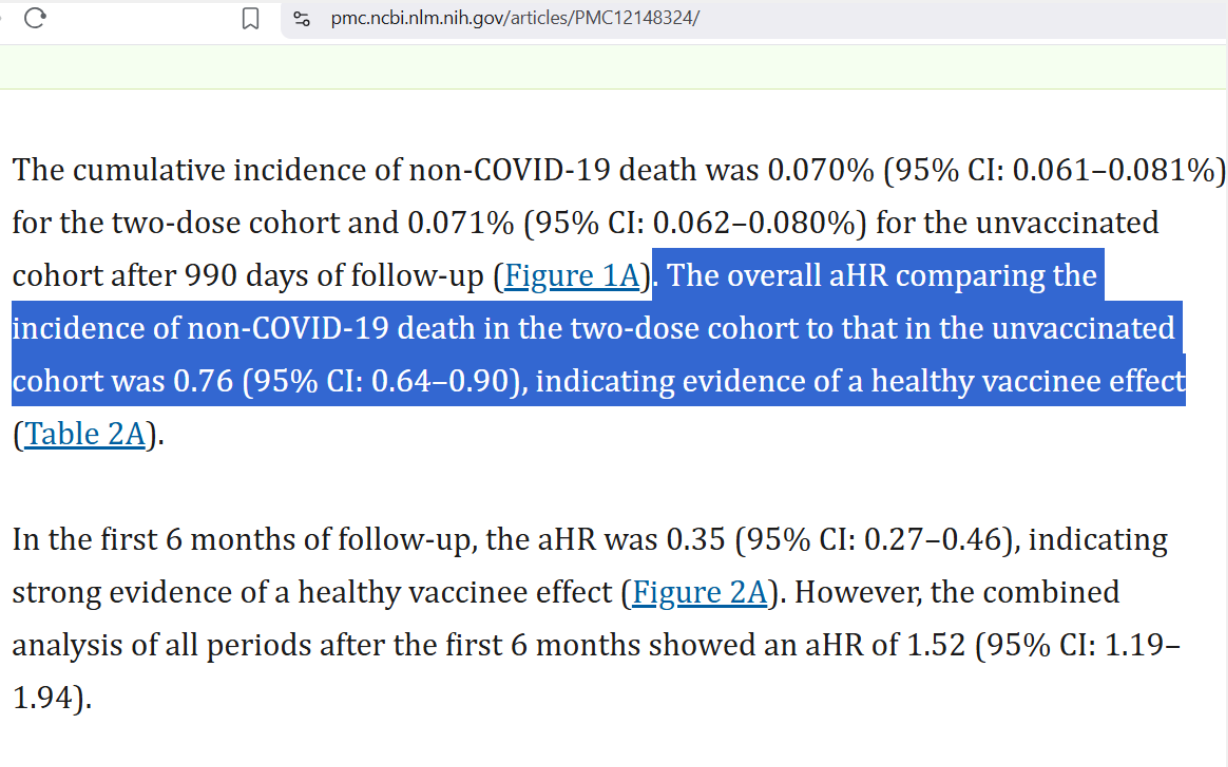
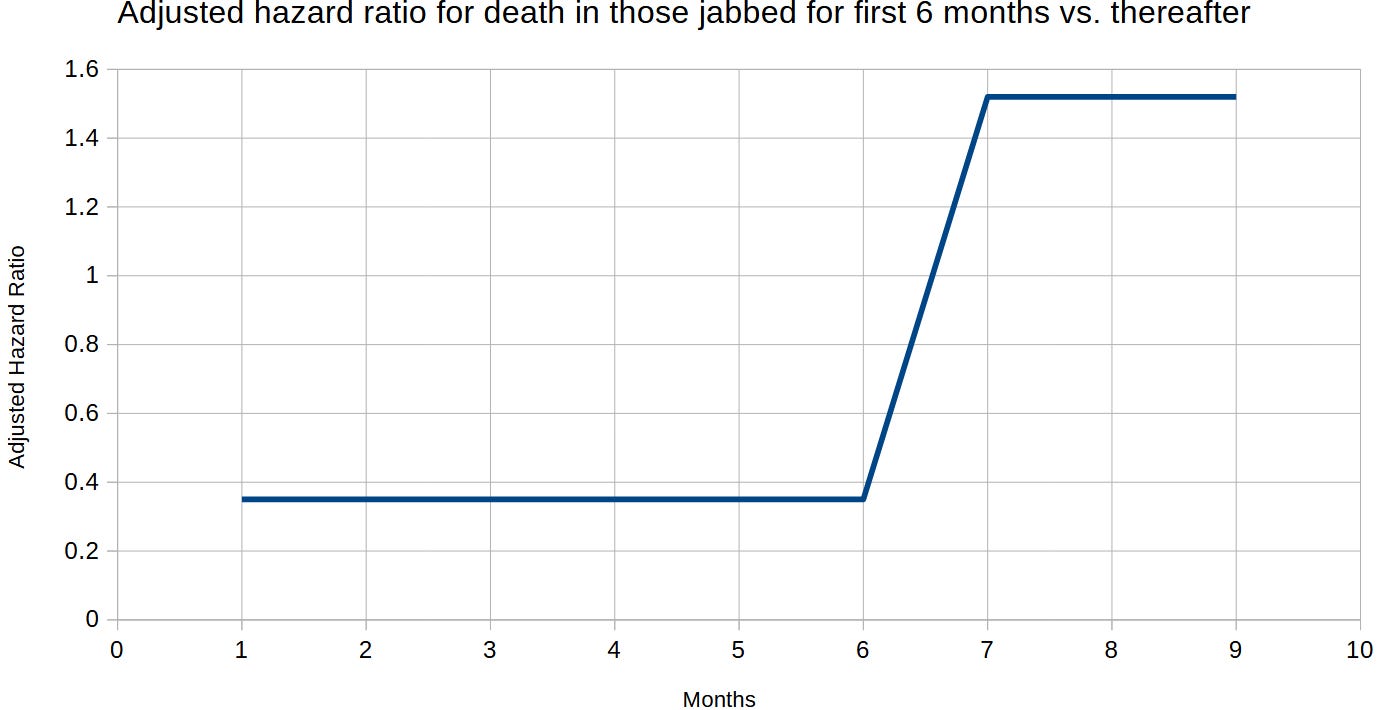
After matching over 800,000 people taking two doses of COVID shots, they found an overall ratio on non-COVID death rate of 0.76 — meaning that those choosing to take COVID shots had an underlying death risk which was (100% - 76% =) 24% lower than those refraining from taking them. So, to find “true” vaccine events, divide by 0.76.
The adjusted hazard ratio in the first 6 months indicated a healthy vaccine bias that was stronger (65%), but the overall estimate is used in order to obtain a minimum. After 6 months, vaccinated people began dying at higher rates from non-COVID causes, despite being healthier people (1.0 = the rate of the unvaccinated):
Applied Example
Applied to a study from Italy, we can verify the excess rate of bladder cancer in the COVID-shot-dosed subjects — under the impression that those in the vaccinated group are going to have a minimum of a 24% risk reduction for morbidity and mortality (the minimum value of a healthy vaccinee effect). Here are the reported original numbers:
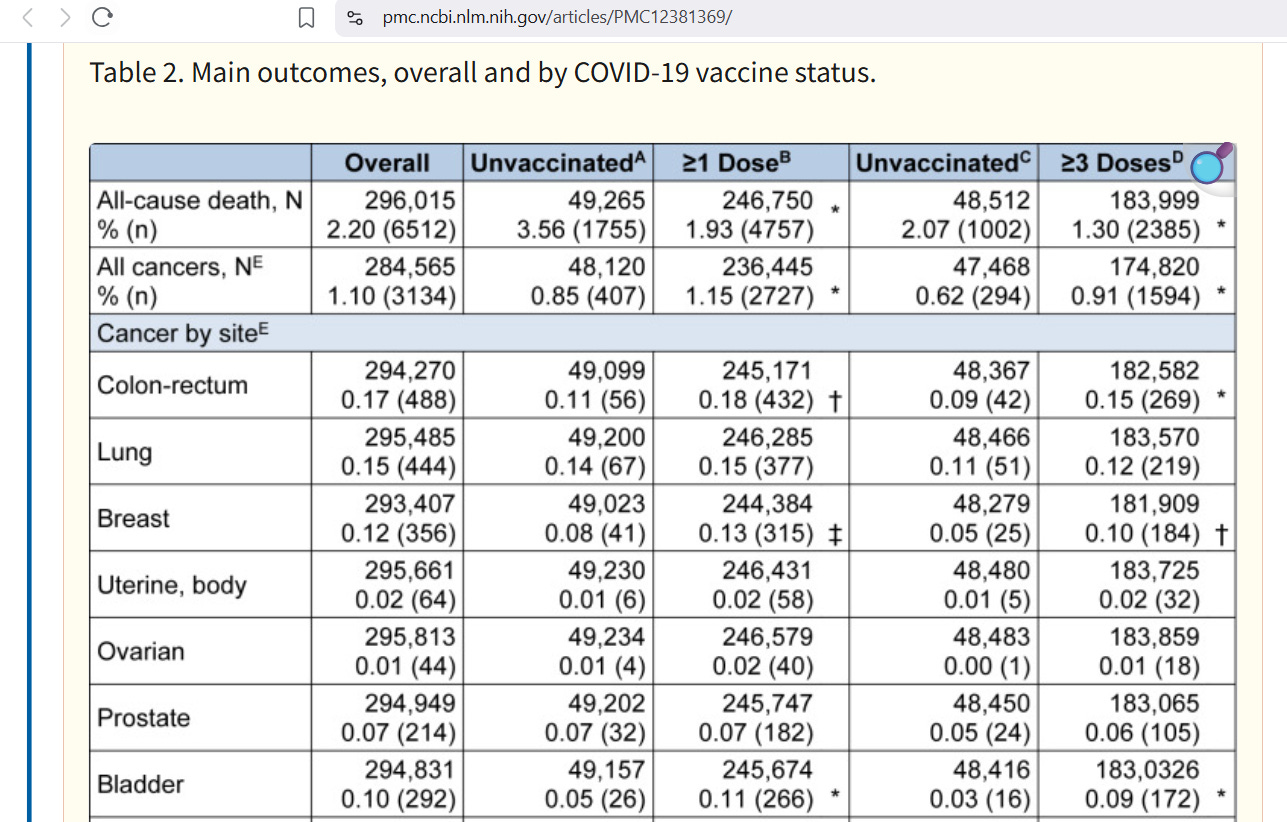
For unvaccinated vs. 1+ Doses, the rate of bladder cancer was 0.05% in those unvaccinated and more than double (0.11%) in those vaccinated. For unvaccinated vs. 3+ Doses, the rate of bladder cancer was 0.03% in those unvaccinated and it was triple (0.09%) in those vaccinated. But this study does not correct for healthy vaccinee bias.
To find out what the real estimate is after correcting for healthy vaccinee bias, you can divide the event count for cancers among the vaccinated groups by 0.76 — as the study in Qatar revealed. Here is what happens when you do that:
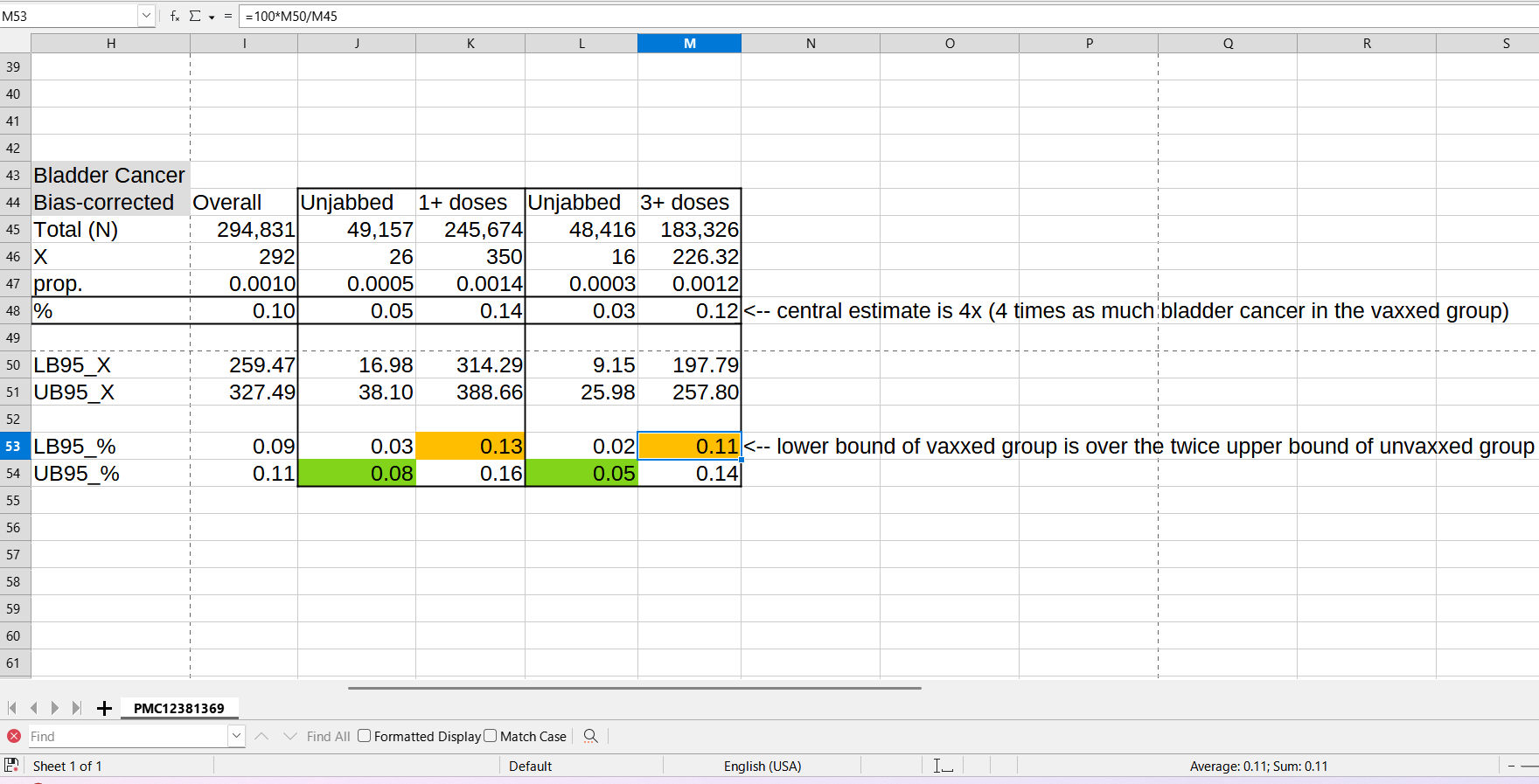
After correcting for the healthy vaccinee bias (using the minimum value of correction), then the risk of bladder cancer rises by 4x after taking three doses of COVID shots — i.e., the primary series plus one booster shot quadruples your risk for bladder cancer.
Reference
[presentation by Tracy Beth Hoeg indicating bias of 41% or more] — https://cdn.who.int/media/docs/default-source/documents/r-d-blueprint-meetings/improvingvaccineeffectivenessmtg/1_2_tracy-hoeg.pdf?sfvrsn=a317585d_3
[small magnitude value of 24% healthy vaccinee bias in Qatar study] — Chemaitelly H, Ayoub HH, Coyle P, Tang P, Hasan MR, Yassine HM, Al Thani AA, Al-Kanaani Z, Al-Kuwari E, Jeremijenko A, Kaleeckal AH, Latif AN, Shaik RM, Abdul-Rahim HF, Nasrallah GK, Al-Kuwari MG, Al-Romaihi HE, Al-Thani MH, Al-Khal A, Bertollini R, Butt AA, Abu-Raddad LJ. Assessing healthy vaccinee effect in COVID-19 vaccine effectiveness studies: a national cohort study in Qatar. Elife. 2025 Jun 9;14:e103690. doi: 10.7554/eLife.103690. PMID: 40488740; PMCID: PMC12148324. https://pmc.ncbi.nlm.nih.gov/articles/PMC12148324/
[Italian cancer risk to be corrected by the minimum healthy vaccinee bias] — Acuti Martellucci C, Capodici A, Soldato G, Fiore M, Zauli E, Carota R, De Benedictis M, Di Marco G, Di Luzio R, Flacco ME, Manzoli L. COVID-19 vaccination, all-cause mortality, and hospitalization for cancer: 30-month cohort study in an Italian province. EXCLI J. 2025 Jul 1;24:690-707. doi: 10.17179/excli2025-8400. PMID: 40881928; PMCID: PMC12381369. https://pmc.ncbi.nlm.nih.gov/articles/PMC12381369/
Do you know if these studies corrected for age?