

Omicron cannot Explain even a Third of Recent Excess Death
Omicron cannot Explain even a Third of Recent Excess Death
Evidence from the UK

When Kaiser Permanente in southern California followed 237,000 cases of Omicron variant (including BA.1 and BA.2), they found 35 total deaths. Across these sublineages, it took 6800 cases of Omicron, just to produce one death.
To give perspective, using a published estimate for asymptomatic proportions, the median flu infection fatality rate (IFR) for 7 recent seasons from 2012/13 to 2018/19 was 0.106% — which translates into one flu death for every 940 flu infections: i.e., the median IFR of recent seasonal flu is approximately 7 times more deadly than Omicron.
If seasonal flu is 7 times more deadly than Omicron, as evidence from following over 200,000 Omicron infections suggests, then why all the recent excess death?
Recent Excess Death in the UK
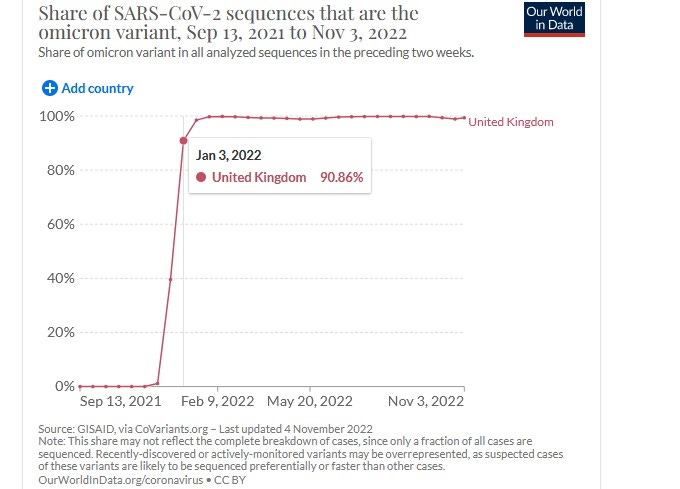
The UK has had Omicron dominance beginning in the first week of January:
Yet excess death estimates for the UK from The Economist are still showing high daily excess death rates in the UK, even exceeding an example of the worst recent flu (2017/18) in the Netherlands, one of the countries hit hardest in 2018:
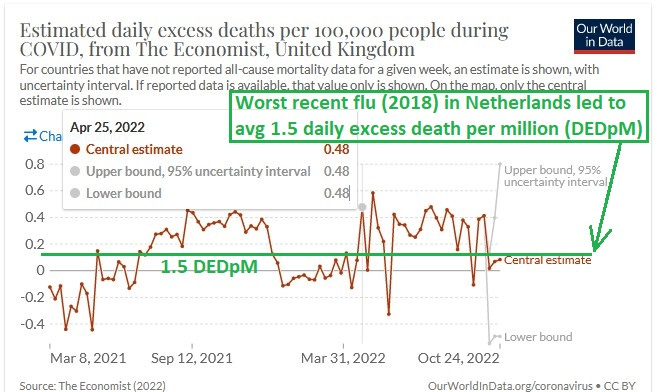
Notice how it is that even late April through late October (“out-of-flu-season”) deaths are running very high. The 25 April 2022 excess death rate showing is 0.48 per 100,000 — or 4.8 daily excess deaths per million.
In the last 6 months, these excess death estimates amount to 35,000 excess deaths in the UK — all during the dominance of a viral disease which is many times safer than flu?
It is even, or maybe especially, happening among those of working age. The working age in England and Wales from 2010-2020 had a peak excess winter mortality (Dec-Mar average death, divided by the average of the other 8 months) of 13%.
But even during summer months in the UK, the rate of excess death among those of working age is even higher than that:

The 21 Aug 2022 estimate of 21% excess mortality among the non-elderly is inexplicable — because August is typically one of the months with the lowest mortality.
Thought Experiment
Let’s try to explain the 35,000 estimated excess deaths in the UK over the last 6 months by ascribing all deaths to Omicron infections. How many infections would be needed in order to create that much excess death?
At 6800 infections per death, the UK would have had to have experienced — over just the last 6 months — 238 million Omicron infections, even though there are only 67 million people living there.
If you do the math, then that is over 3.5 infections per man, woman, and child within 6 months (more than one new infection in each and every person every two months).
Evidence from Denmark suggests that it is possible for about two-thirds of the population to become infected in just over 4 months. Applied to the UK, that'd mean 44 million Omicron infections — enough to kill 6,500 people out of the 35,000 excess deaths noted above.
That’s not even 20% of the excess deaths though, which suggests that over 80% of all recent excess deaths need to be explained.
A Rough Guess
A rough guess is that about a third of unexplained excess death will be explained by the medium- and long-term effects of strict COVID countermeasures such as masks and lockdowns.
With people postponing cancer screenings, experiencing mental health breakdowns, and subjecting themselves to bacterial superconcentration from long-duration mask use — much morbidity and mortality is expected.
A prime candidate for the other two-thirds of unexplained excess death would be the experimental COVID shots. COVID itself can no longer explain even a third of recent excess death, but something must be causing it.
Reference
[6800 Omicron infections to produce one single death; join data from tables S12 and S14 in the supplement to get the overall average] — Lewnard JA, Hong VX, Patel MM, Kahn R, Lipsitch M, Tartof SY. Clinical outcomes associated with SARS-CoV-2 Omicron (B.1.1.529) variant and BA.1/BA.1.1 or BA.2 subvariant infection in Southern California. Nat Med. 2022 Sep;28(9):1933-1943. doi: 10.1038/s41591-022-01887-z. Epub 2022 Jun 8. PMID: 35675841. https://doi.org/10.1038/s41591-022-01887-z
[CDC page on Burden of Flu] — CDC. https://www.cdc.gov/flu/about/burden/index.html
[16% of all flu infections remain asymptomatic; 84% of them progress to symptoms] — Leung NH, Xu C, Ip DK, Cowling BJ. Review Article: The Fraction of Influenza Virus Infections That Are Asymptomatic: A Systematic Review and Meta-analysis. Epidemiology. 2015 Nov;26(6):862-72. doi: 10.1097/EDE.0000000000000340. PMID: 26133025; PMCID: PMC4586318. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4586318/
[average daily excess death during 2018 in the Netherlands was 1.5 per million; peak daily death was 9.9 per million] — van Asten L, Harmsen CN, Stoeldraijer L, Klinkenberg D, Teirlinck AC, de Lange MMA, Meijer A, van de Kassteele J, van Gageldonk-Lafeber AB, van den Hof S, van der Hoek W. Excess Deaths during Influenza and Coronavirus Disease and Infection-Fatality Rate for Severe Acute Respiratory Syndrome Coronavirus 2, the Netherlands. Emerg Infect Dis. 2021 Feb;27(2):411-420. doi: 10.3201/eid2702.202999. Epub 2021 Jan 4. PMID: 33395381; PMCID: PMC7853586. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7853586/
[age-specific Excess Winter Mortality; Table 2] — Jones RP. Excess Winter Mortality (EWM) as a Dynamic Forensic Tool: Where, When, Which Conditions, Gender, Ethnicity and Age. Int J Environ Res Public Health. 2021 Feb 23;18(4):2161. doi: 10.3390/ijerph18042161. PMID: 33672133; PMCID: PMC7926905. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7926905/
[two-thirds of Denmark infected in just over 4 months of time] — Erikstrup C, Laksafoss AD, Gladov J, Kaspersen KA, Mikkelsen S, Hindhede L, Boldsen JK, Jørgensen SW, Ethelberg S, Holm DK, Bruun MT, Nissen J, Schwinn M, Brodersen T, Mikkelsen C, Sækmose SG, Sørensen E, Harritshøj LH, Aagaard B, Dinh KM, Busch MP, Jørgensen CS, Krause TG, Ullum H, Ostrowski SR, Espenhain L, Pedersen OBV. Seroprevalence and infection fatality rate of the SARS-CoV-2 Omicron variant in Denmark: A nationwide serosurveillance study. Lancet Reg Health Eur. 2022 Oct;21:100479. doi: 10.1016/j.lanepe.2022.100479. Epub 2022 Aug 5. PMID: 35959415; PMCID: PMC9355516. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9355516/
[Extended mask use more than triples the concentration of bacteria on the inside of the mask] — Zhiqing L, Yongyun C, Wenxiang C, Mengning Y, Yuanqing M, Zhenan Z, Haishan W, Jie Z, Kerong D, Huiwu L, Fengxiang L, Zanjing Z. Surgical masks as source of bacterial contamination during operative procedures. J Orthop Translat. 2018 Jun 27;14:57-62. doi: 10.1016/j.jot.2018.06.002. PMID: 30035033; PMCID: PMC6037910. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6037910/
[Extended mask use more the triples the bacterial concentration on the face] — Marín-Nieto J, Reino-Perez C, Santillana-Cernuda G, Díaz-Bernal JM, Luque-Aranda R, García-Basterra I. FACE MASK CONTAMINATION DURING COVID-19 PANDEMIA. A STUDY ON PATIENTS RECEIVING INTRAVITREAL INJECTIONS. Retina. 2021 Nov 1;41(11):2215-2220. doi: 10.1097/IAE.0000000000003202. PMID: 33965993. https://pubmed.ncbi.nlm.nih.gov/33965993/