

World War II (WWII) was a pretty bad war as far as wars go. Almost 300,000 Americans ended up dying during WWII. Because it was protacted, the actual monthly rate of death per million was slightly lower than that seen for WWI — when “only” 117,000 Americans died.
It was a time when adversaries admitted that they are at war with you, so there was no need to check the excess death rate in order to statistically determine if your nation is experiencing a war — because the excess death rate had exceeded the limits of variability regarding death by natural causes.
As I detailed here, COVID deaths for the 24 months from March 2020 to March 2021 ran somewhere from 100,000 up to 400,000 in total — though the CDC is fond of reporting different death numbers (numbers which cannot be backed by science). Here is a graph that shows how the low and the high estimates of COVID deaths compare to WWII:
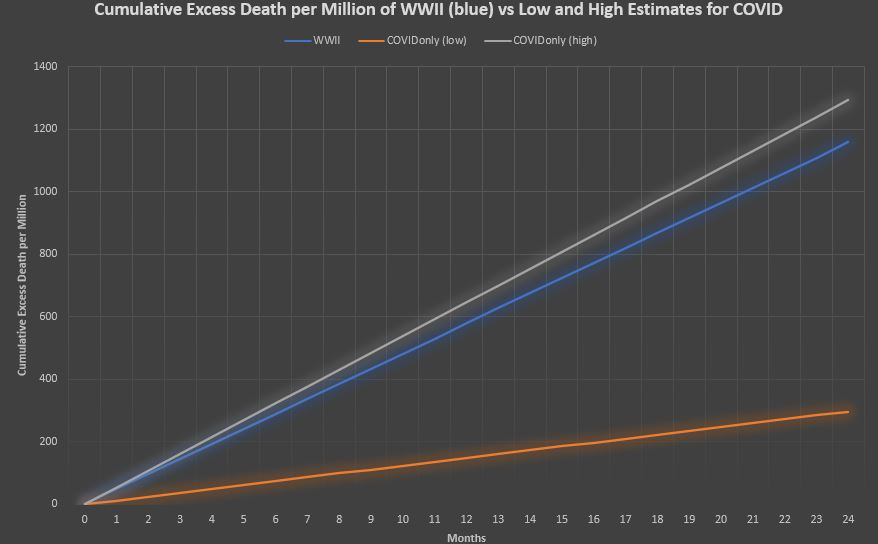
The bottom orange line is the best-case scenario infection fatality rate (IFR) for 4 variants of COVID (Wuhan1, Alpha, Delta, Omicron) along with the assumption that total COVID infections in the USA were always exactly twice what the confirmed case counts were.
Evidence suggests that it’s unreasonable to imagine COVID infections which were less than twice the COVID case count. To my knowledge, no nation has published evidence indicating that they successfully confirmed over half of all background COVID infections.
The blue line is the average monthly death rate for WWII — 48.3 monthly deaths per million (MDpM) — accumulating evenly over time, even if they didn’t accrue so evenly, for the purpose of clear presentation.
The top gray line is the worst-case scenario IFR for each of the 4 COVID variants (Wuhan1, Alpha, Delta, Omicron), along with the assumption that total COVID infections in the USA were always 5 times what the confirmed case counts were.
Evidence suggests that it’s unreasonable to imagine COVID infections which were over 5 times more than the COVID case count — though isolated trials have been able to produce it by looking at nations which did not have broad testing campaigns.
But the USA was not one of those nations which failed to have a broad COVID testing campaign, so it is not reasonable to entertain notions about COVID infection incidence being higher than 5 times the confirmed cases.
What about non-COVID excess death?
If COVID only explains 15% to 30% of the actual excess deaths which have occurred in the USA, then what about the other 70% to 85% of the excess deaths which have occurred?
Here is a graph showing those excess deaths as compared to the excess deaths seen during WWII:
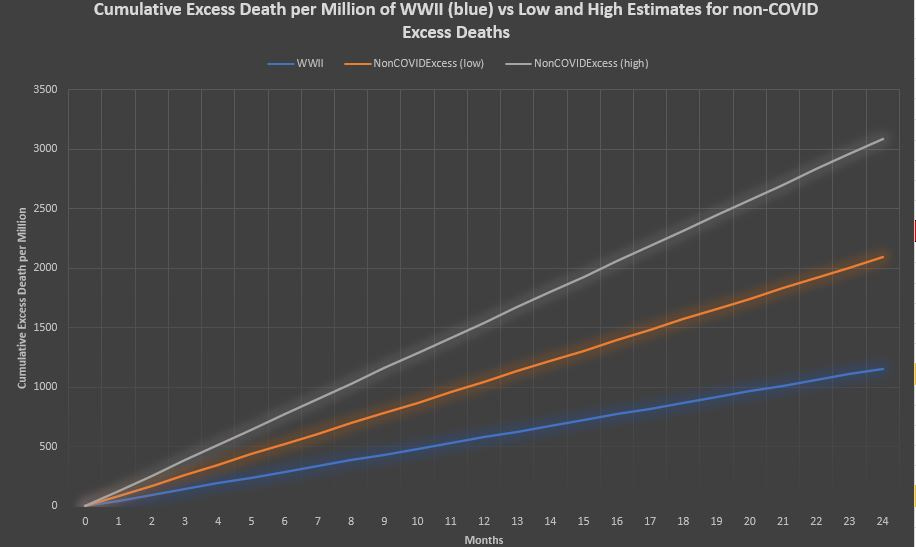
The blue line still represents WWII excess deaths here, but now even the low estimate of non-COVID excess death is above the death rate seen during world war.
The high estimate for non-COVID excess deaths coincides with the low estimate for COVID deaths — where COVID deaths were 100,000, but non-COVID excess deaths were another million on top of that.
At that high estimate, non-COVID excess deaths were already over twice as bad as a world war. Let’s look at the all-cause excess death rate in the USA compared to WWII:
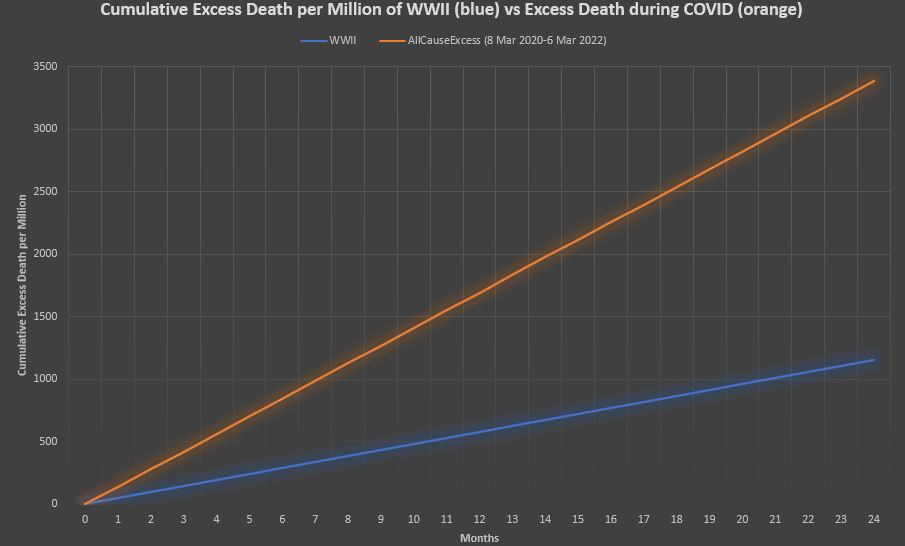
WWII is still the blue line and now the total of all excess death for 24 months shows that excess deaths during COVID accrued at a rate that is 2.9 times faster than a world war.
The excess deaths during COVID are going to go down in the history books. Even including early smallpox epidemics in America, the only other time in all of American history when Americans died at the excess rate that they’ve died recently, was during the Civil War.
In order to get death rates THIS high, you cannot rely on natural causes like diseases. Natural causes do not fluctuate enough to cause this high of an excess death rate.
Critics and detractors may point to Spanish Flu, and for good reason. World excess death rates associated with Spanish Flu, excluding India, were 4870 per million in 1918 and 1010 per million in 1919.
It looks like, this time, the critics and detractors have me painted into a corner …
More people died then because they were accidentally doing the wrong things
But to split hairs, most of the excess death associated with Spanish Flu was not from Spanish Flu, but rather from bacterial superinfection likely tied to the excess wearing of facemasks in 1918 and 1919 (which superconcentrates bacteria counts in the mouth, nose, and throat).
That puts the Spanish Flu death rate at most at 2435 per million for 1918, and at most at 505 per million for 1919. Added together, that’s 2940 per million over the course of two years — and even the high estimate of the non-COVID death rate (3090 per million) was higher than the (Spanish Flu-only) death rate.
The all-cause excess death rate from March 2020 to Mar 2022 (3387 per million) was definitely higher than the two-year (Spanish Flu-only) excess death rate of 2940 per million.
Spanish Flu was a natural-caused death, but “masking up” and superconcentrating bacteria — so that you end up dying from bacterial pneumonia — is more correctly labelled as an external cause of death (accidents, suicides, homicides).
In order to get death rates this high, you have to have a nation that is at war with itself.
This is so that the extra death by external causes (accidents, suicides, homicides) can add to the extra death by natural causes such as diseases. Diseases alone (natural causes) do not cause the kind of death which was seen in the USA from March 2020 to March 2022.
Reference
[Cumulative Excess Mortality during COVID-19] — OurWorldInData [Human Mortality Database data]. https://ourworldindata.org/excess-mortality-covid
[Encyclopedia Britannica on WWII losses for USA of 298,000] — https://www.britannica.com/event/World-War-II/Costs-of-the-war
[mid-war (avg of 1943 and 1944) US population of 137.6 million] — U.S. Bureau of Economic Analysis, Population [B230RC0A052NBEA], retrieved from FRED, Federal Reserve Bank of St. Louis; https://fred.stlouisfed.org/series/B230RC0A052NBEA
[Excess death rate due to Spanish Flu, excluding India, was 4870 per million in 1918 and 1010 per million in 1919] — Spreeuwenberg P, Kroneman M, Paget J. Reassessing the Global Mortality Burden of the 1918 Influenza Pandemic. Am J Epidemiol. 2018 Dec 1;187(12):2561-2567. doi: 10.1093/aje/kwy191. PMID: 30202996; PMCID: PMC7314216. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7314216/
[most Spanish Flu deaths were not even from the Spanish Flu] — Morens DM, Taubenberger JK, Fauci AS. Predominant role of bacterial pneumonia as a cause of death in pandemic influenza: implications for pandemic influenza preparedness. J Infect Dis. 2008 Oct 1;198(7):962-70. doi: 10.1086/591708. PMID: 18710327; PMCID: PMC2599911. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2599911/
[Extended mask use more than triples the concentration of bacteria on the inside of the mask] — Zhiqing L, Yongyun C, Wenxiang C, Mengning Y, Yuanqing M, Zhenan Z, Haishan W, Jie Z, Kerong D, Huiwu L, Fengxiang L, Zanjing Z. Surgical masks as source of bacterial contamination during operative procedures. J Orthop Translat. 2018 Jun 27;14:57-62. doi: 10.1016/j.jot.2018.06.002. PMID: 30035033; PMCID: PMC6037910. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6037910/
[Extended mask use more the triples the bacterial concentration on the face] — Marín-Nieto J, Reino-Perez C, Santillana-Cernuda G, Díaz-Bernal JM, Luque-Aranda R, García-Basterra I. FACE MASK CONTAMINATION DURING COVID-19 PANDEMIA. A STUDY ON PATIENTS RECEIVING INTRAVITREAL INJECTIONS. Retina. 2021 Nov 1;41(11):2215-2220. doi: 10.1097/IAE.0000000000003202. PMID: 33965993. https://pubmed.ncbi.nlm.nih.gov/33965993/