
Provably Counter-productive by Month 4
Post #1083

NOTE: Due to adverse effects of COVID shots, they would be required to provide significant benefits in order to offset the negative effects. Failure to provide significant benefit is therefore evidence of net harm from them.
It is difficult to prove that COVID shots were counter-productive in the first 3 months that they were given, but by the 4th month after the rollout, it was no longer difficult to prove that COVID shots were counter-productive. Vaccinating into a pandemic is bad because there is a chance of immune-imprinting, or Original Antigenic Sin (OAS):

[click to enlarge]
Notice how advice is given near the bottom to not create a vaccine that targets a specific disease (acquired, antibody-based immunity), but to instead use compounds to boost innate, non-specific (cell-mediated) immunity. Though the COVID shot was based on the original Wuhan-1 strain, by 12 Apr 2021, that strain was no longer dominant:

The purple area is for Alpha variant, comprising 61% of all identified variants. This means that wild-type (Wuhan-1) was knocked from the top. There is a thin blue line between the green area and the gray area at right and, can you guess what that variant is?
That’s right, it’s Delta variant, and that’s just 4 months in, and it was already poised to become the third dominant variant in the first 6 months of COVID shots. Here is right before Delta variant took off to become the dominant variant:

By 7 Jun 2021 it was at 14% and rising quickly. But if you get a new dominant variant every 2 to 3 months and you go ahead and attempt to vaccinate — then you risk the “ineffective immune response against the mutated virus due to OAS” that was warned about above. Vaccines are expected to fail in cases when new variants arise quickly.
For SARS-CoV-2, confirmation of onward transmission would involve 3 measures, viral RNA (vRNA), recovery of the infectious virus (growing it in cells in a lab, after extracting it from a sample taken from the infected person), and seroconversion, where you develop antibodies that are reactive to the antigens of the specific pathogen:

An argument can be made that the most important one is “recovery of infectious virus” — because it verifies the potential for that person to be another link in the chain of onward transmission. For Alpha and Delta, recovery of infectious virus from those who took the COVID shots (vs. those who did not) revealed no COVID shot efficacy:

At top left are Ct values, and the lower they go, the more virus you have in you. When comparing the averages (horizontal lines) between adjacent groups (unjabbed, then jabbed), the lines for those who took COVID shots were nominally lower — meaning that those who took COVID shots had more of the virus growing inside of them.
The header at top where it says “CPE positive” designates those from whom the samples led to confirmation of infectious virus. Data points trend lower on that side, as would be expected, because lower Ct values mean higher viral loads. At bottom, red sections show the proportion of samples with infectious virus. Look at Delta though.
For those who remained unjabbed, Delta infections led to 96.7% of samples containing infectious virus but — for those who took COVID shots — an alarming 100% of samples contained infectious virus (every recipient of COVID shots, once infected, become a potential link in the chain of onward transmission, i.e., a spreader):

The nominally-higher proportion of infectious virus from those who took COVID shots means that there is a documented failure to provide significant benefit, which was required, because of the significant adverse effects they cause. Having a proportion of 100% who have infectious virus makes the shots counter-productive.
It doesn’t make medical sense to “vaccinate” against a disease that has a new dominant variant every 2 or 3 months. If immune imprinting occurs, then it can even be dangerous. It is better to protect yourself by boosting non-specific immunity, by eating clean, exercising, resting, and getting good nutrition (e.g., more protein, less sugar).
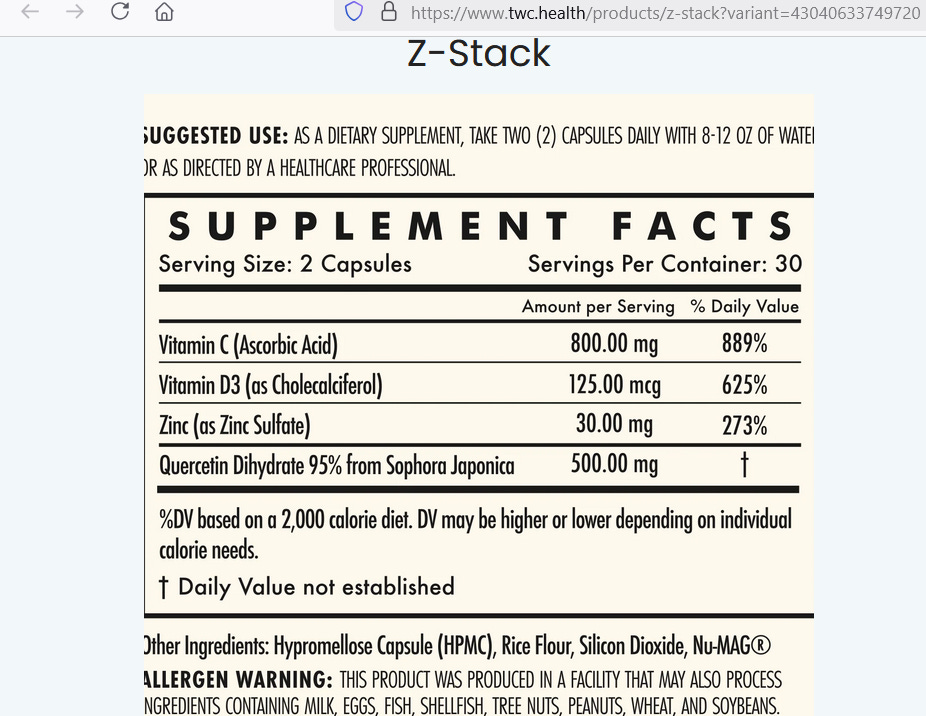
To super-charge your immunity, a good product is Z-Stack, put out by The Wellness Company:
Reference
[vaccines can work against you when new variants come along] — Roncati L, Palmieri B. What about the original antigenic sin of the humans versus SARS-CoV-2? Med Hypotheses. 2020 Sep;142:109824. doi: 10.1016/j.mehy.2020.109824. Epub 2020 May 7. PMID: 32408068; PMCID: PMC7204740. https://pmc.ncbi.nlm.nih.gov/articles/PMC7204740/
[three-way verification of onward transmission of a communicable disease] — Patel DR, Field CJ, Septer KM, Sim DG, Jones MJ, Heinly TA, Vanderford TH, McGraw EA, Sutton TC. Transmission and Protection against Reinfection in the Ferret Model with the SARS-CoV-2 USA-WA1/2020 Reference Isolate. J Virol. 2021 Jun 10;95(13):e0223220. doi: 10.1128/JVI.02232-20. Epub 2021 Jun 10. PMID: 33827954; PMCID: PMC8315962. https://pmc.ncbi.nlm.nih.gov/articles/PMC8315962/
[COVID shots led to nominally higher viral loads and nominally higher proportion of recoverable infectious virus when applied to Delta variant] — Huai Luo C, Paul Morris C, Sachithanandham J, Amadi A, Gaston DC, Li M, Swanson NJ, Schwartz M, Klein EY, Pekosz A, Mostafa HH. Infection With the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Delta Variant Is Associated With Higher Recovery of Infectious Virus Compared to the Alpha Variant in Both Unvaccinated and Vaccinated Individuals. Clin Infect Dis. 2022 Aug 24;75(1):e715-e725. doi: 10.1093/cid/ciab986. PMID: 34922338; PMCID: PMC8903351. https://pmc.ncbi.nlm.nih.gov/articles/PMC8903351/