

The Iatrogenic Hypothesis of Neil and Fenton
The Iatrogenic Hypothesis of Neil and Fenton
The seeming impossibility of COVID death numbers

Over at the Substack of
, Neil and Fenton make a very strong case that the main reason for high excess death is the quality of medical care, and not the inherent lethality of an acute respiratory disease called COVID.When compared against the age-based lethality of other respiratory diseases, COVID is in the middle of the pack:

Here is the graph but with some notes added into it:

When researchers compared the age-specific infection fatality rate (IFR) of COVID versus flu, they found fatality risk rising exponentially after age 40: at 10.7% per year after age 40 for COVID, and 8.5% per year after age 40 for flu.
Using updated COVID (original Wuhan-1 strain) IFR data from Ioannidis, and adjusting the age 45 IFR to represent the higher risk of flu for that age, I made this comparison:
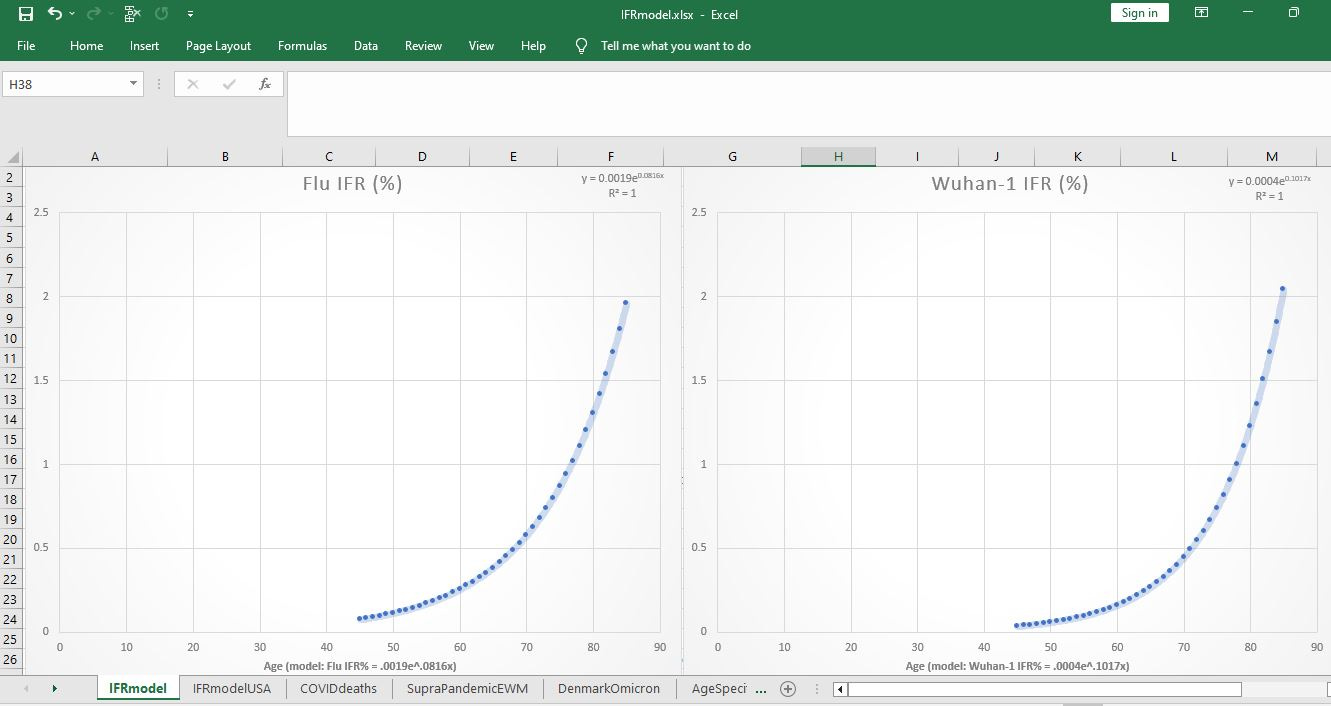
[click image to enlarge]
Age is across the bottom and flu is at left. You can tell that the death risk of flu infection at age 45 is higher than that for Wuhan-1 COVID at right. But then COVID gets more deadly than flu for a 25-year age span, until finally — after age 80 — there is no discernible difference between COVID and flu.
After age 80, they are functionally equivalent.
But if COVID was never over twice as bad as flu, how could it be the case that, in 3 months in New York, there were 31,000 “COVID deaths”?

Notice the week of 11 Apr 2020, where there were 6,634 COVID deaths in 7 days. If New York flu deaths, even in severe flu seasons, never even reach 5,000 — then how can it be the case that over 6 times as much COVID death was seen than in severe flu?
How can it be the case that, in one week, COVID caused more deaths (6,634) than severe flu does in 52 weeks (4,881)?

The best explanation for the excess deaths is the implementation of low-quality (unsound) medical practices in the state of New York, and presumably elsewhere.
Early treatment, as advised by Dr. Peter McCullough and others, was not performed. Promising therapies such as vitamin C, vitamin D, zinc, ivermectin, and hydroxychloroquine were not used.
The upshot is: When you don’t use the best tools in your toolkit, then don’t expect to fix the problem. In fact, the widespread (“regimented”) use of sub-optimal medical practices is what best explains the excess deaths that were seen.
Reference
[both flu and COVID risk rise exponentially with age, from age 40 onwards] — Comparing the age and sex trajectories of SARS-CoV-2 morbidity and mortality with other respiratory pathogens. C. Jessica E. Metcalf, Juliette Paireau, Megan O'Driscoll, Mathilde Pivette, Bruno Hubert, Isabelle Pontais, Sema Nickbakhsh, Derek A. T. Cummings, Simon Cauchemez, and Henrik Salje. Published: 15 June 2022. https://doi.org/10.1098/rsos.211498
[Wuhan-1 IFR for those in their 40's is 0.035%] — Pezzullo AM, Axfors C, Contopoulos-Ioannidis DG, Apostolatos A, Ioannidis JPA. Age-stratified infection fatality rate of COVID-19 in the non-elderly population. Environ Res. 2023 Jan 1;216(Pt 3):114655. doi: 10.1016/j.envres.2022.114655. Epub 2022 Oct 28. PMID: 36341800; PMCID: PMC9613797. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9613797/