

Unexpected Trend in New York ICU Beds
Unexpected Trend in New York ICU Beds
Early 2020 data

In this previous Substack, it was discovered that New York was never short on hospital beds — so that there was never a need to have an expensive Navy medical ship sitting in port. A second disturbing aspect from researching for that article is reported here.
If you expand your ICU bed capacity, you typically do so so that you will have less strain on your resources. But when New York counties expanded their ICU bed capacities, something else happened, instead:
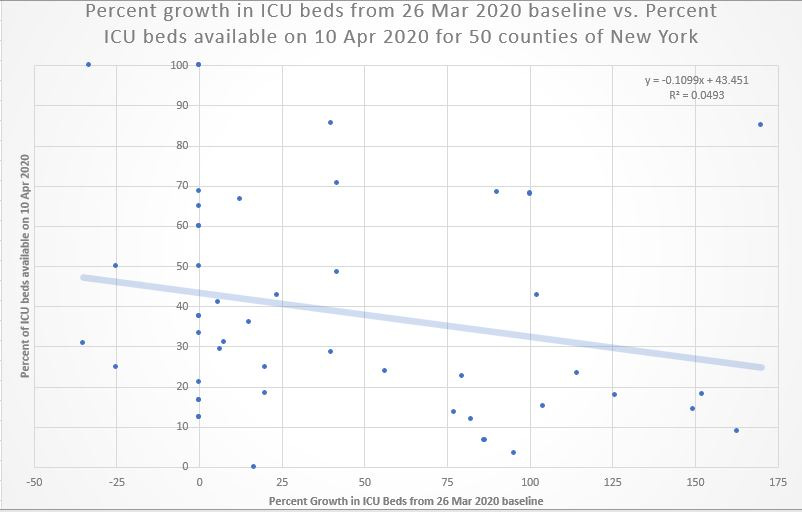
The horizontal (X) axis shows the percentage expansion in ICU bed capacity by county from a baseline of 26 Mar 2020 up to 10 Apr 2020. In counties that didn’t expand their ICU bed capacity, the expectation for 10 Apr 2020 would be that they’d have 43.5% of the ICU beds available (the Y-intercept when the X-axis is at zero).
But counties expanding their baseline ICU capacity by more than 125% would be expected to have less than 30% of their ICU beds available. Expanding your capacity meant having less residual capacity left over on 10 Apr 2020.
Emergency Medical Care should be different
There is a saying in supply-side economics: “If you build it, they will come” but that aspect of economics should not apply to emergency medical care. Following the logic, it’d mean that tripling the amount of emergency rooms would triple the amount of life-threatening accidents.
With much more emergency rooms built, people would experience much more medical emergencies — just like that. But that’s absurd. Supply-side economics is not supposed to apply to emergency medical care.
A stronger analogy would be funeral homes. With 3 times as many funeral homes, would people begin to die at 3 times the typical rate?
Because “dying” is not something economists call a “normal good” — something you want more of when your access to it increases — funeral home expansion should not increase human death rates.
A virus with a will of its own?
It’s almost as if coronavirus “knew” where the ICU capacity had been expanded, and it “decided” to hit those areas the hardest, leaving the areas that didn’t expand less ravaged.
Critics and detractors may argue that the regression above is weak and statistically insignificant. But a Fisher Exact test (using an online tool) on those counties which expanded their ICU bed capacity by 80% or more shows that they were more likely to be low on ICU bed capacity on 10 Apr 2020:
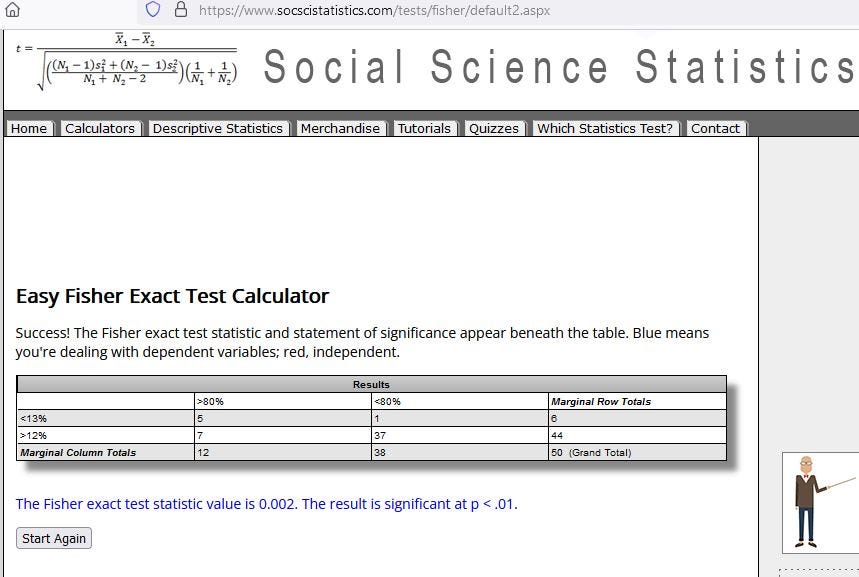
As you can see in the table, 5 of 12 counties with large (80%+) expansion in ICU beds had less than 13% bed availability on 10 Apr 2020 — an arbitrary threshold indicating strain on hospital resources. These are illustrated at bottom right in the scatterplot.
The worst county was Bronx County, with 163% ICU bed capacity expansion, but only 9% bed availability on 10 Apr 2020.
However, only 1 out of the 38 counties which didn’t expand ICU capacity by so much — i.e., Columbia County, with only 7 total ICU beds (lowest dot in scatterplot) — ended up having less than 13% bed availability on 10 Apr 2020.
Reference
[New York hospital bed capacity by county] — https://coronavirus.health.ny.gov/hospital-bed-capacity
Money always exerts an influence. Hence the need for a vaccine and the use of remdesivir.