
Unexpectedly High Excess Death
Comparison of 7-week Time Periods

Vaccine uptake rates have waxed and waned, but you can examine the excess death which went along with the higher rates of vaccination, and compare it to the excess death which was found during lower rates of vaccine administration.
Omicron variant became dominant worldwide approximately on 10 Jan 2022, so you can synchronize the vaccine uptake rate against the corresponding time period in the year prior.
Here is “large-nation” evidence that Omicron (red) was dominant after 10 Jan 2022, successfully replacing Delta variant (blue):
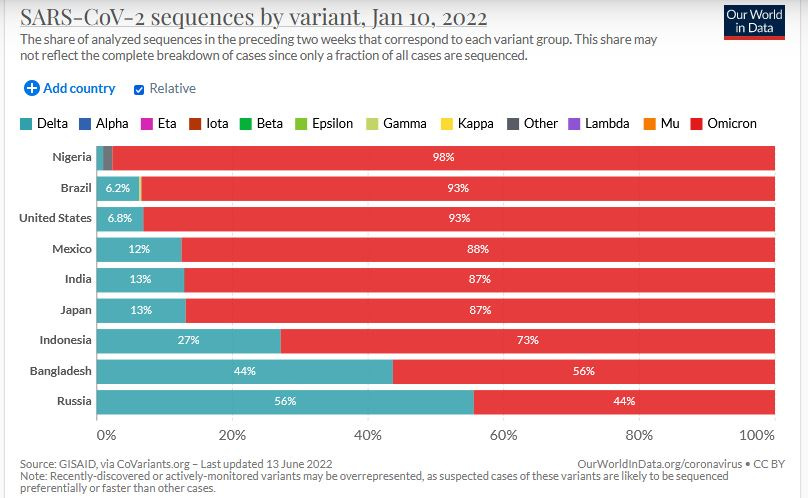
The sum of just the populations of the 9 nations showing above is already in the billions. Because Omicron is so much less lethal than variants before, such as Alpha variant COVID, it can be projected that excess death rates after 10 Jan 2022 would drop like a stone.
Here is a graph showing by how much Omicron is less lethal than the pre-Delta variant of COVID known as Alpha variant:
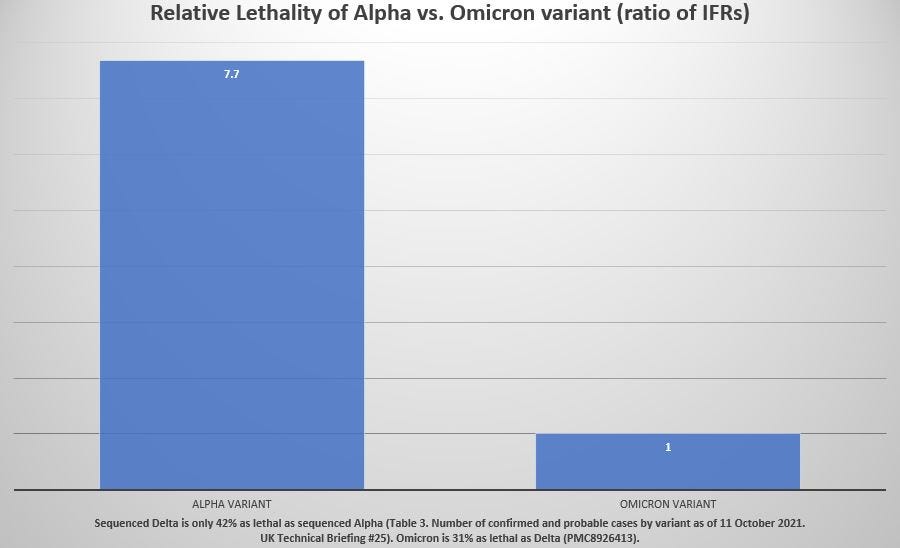
Earlier variants of COVID were more than 7 times more lethal than Omicron variant.
The drop in lethality from Alpha to Delta was 58%, according to the outcomes of 700,000 sequenced COVID infections in Table 3 of Technical Briefing No. 25 from the UK.
The drop in lethality from Delta to Omicron was even more steep than it was when stepping down from Alpha to Delta: Omicron is only 31% as fatal as Delta variant COVID (a 69% drop in the infection fatality rate).
Expected excess death after 10 Jan 2022 should be not even one-seventh of the excess death in the corresponding weeks exactly one year prior. Additional indication that excess deaths should have been practically eliminated by 10 Jan 2022 comes from the rate of vaccine administration.
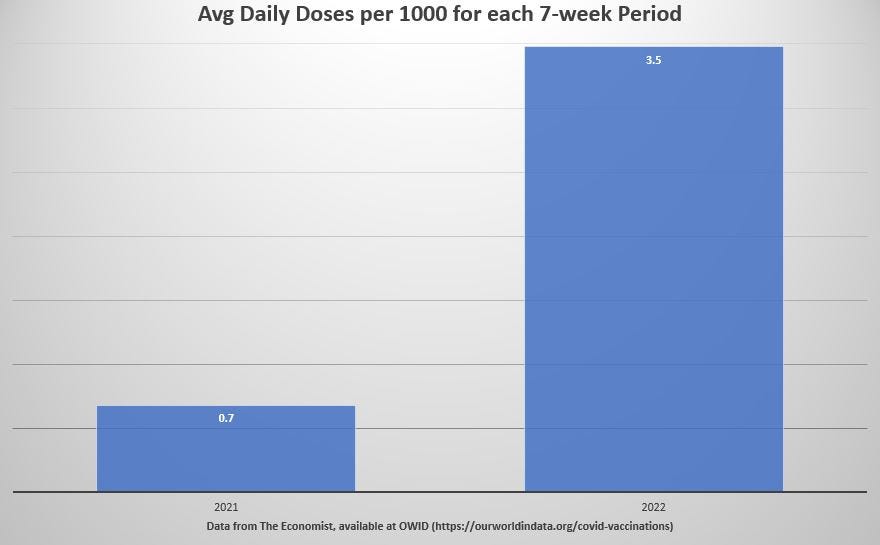
For the 7 weeks from 10 Jan 2022 to 28 Feb 2022, the rate of vaccine administration was more than 3 people per 1000 each day — a rate so high that everyone on planet Earth would be jabbed in under a year (by Day 286, to be more precise).
But not even 1 person in 1000 was getting jabbed per day back in those same weeks of 2021:
So those are two reasons to expect the virtual elimination of all excess death worldwide after 10 Jan 2022. But that expectation did not come true. In fact, precisely the opposite occurred. As COVID got weaker, and as vaccine administration soared, excess deaths rose even higher than their median rate prior to vaccines:
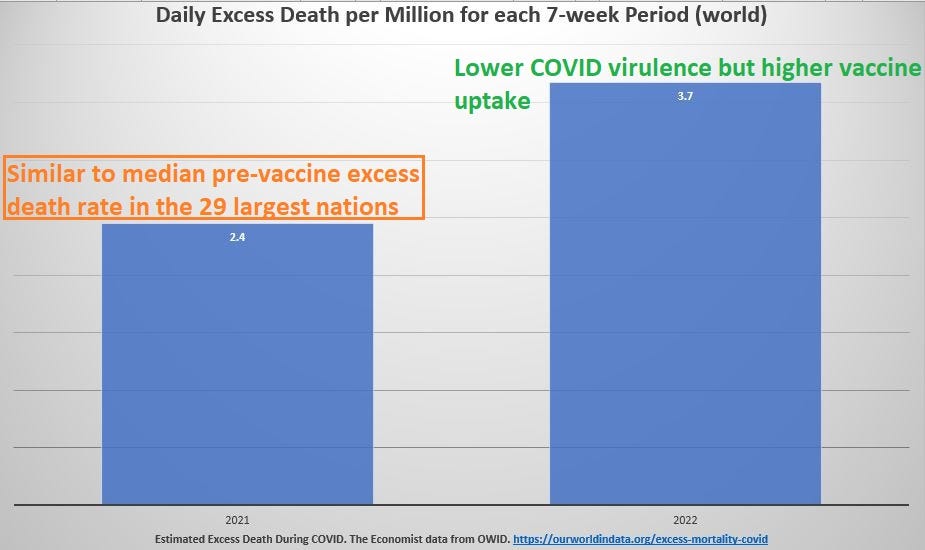
How come it is that when COVID is less lethal, but vaccine administration is high, that excess death rises?
The most plausible answer for having more death when the disease is less fatal is that the vaccines themselves are causing the excess death, rather than the disease.
Reference
[Coronavirus sequences by variant] -- OWID. https://ourworldindata.org/covid-cases
[Total Vaccine doses administered per 100 people] -- OWID. https://ourworldindata.org/covid-vaccinations
[Estimated Cumulative Excess Death during COVID] — The Economist data. OWID. https://ourworldindata.org/excess-mortality-covid
[In almost 700,000 cases confirmed by sequencing, Delta was only 42% as lethal as Alpha] — Table 3. Number of confirmed and probable cases by variant as of 11 October 2021. UK Technical Briefing #25. General page: https://www.gov.uk/government/publications/investigation-of-sars-cov-2-variants-technical-briefings
Available specific page: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1025827/Technical_Briefing_25.pdf
[From 1.5 million confirmed cases, Omicron is 31% as lethal as Delta, making Omicron much safer than the seasonal flu] — Nyberg T, Ferguson NM, Nash SG, Webster HH, Flaxman S, Andrews N, Hinsley W, Bernal JL, Kall M, Bhatt S, Blomquist P, Zaidi A, Volz E, Aziz NA, Harman K, Funk S, Abbott S; COVID-19 Genomics UK (COG-UK) consortium, Hope R, Charlett A, Chand M, Ghani AC, Seaman SR, Dabrera G, De Angelis D, Presanis AM, Thelwall S. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022 Mar 16:S0140-6736(22)00462-7. doi: 10.1016/S0140-6736(22)00462-7. Epub ahead of print. PMID: 35305296; PMCID: PMC8926413. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8926413/