

Updated Risk:Benefit for COVID jabs
Updated Risk:Benefit for COVID jabs
Incorporating an 87% reduction in infection fatality with Omicron

Finding a risk and a benefit is part of implementing good practices in medicine. One outfit that looks for both risks and benefits using evidence-based medicine is The NNT — which uses the acronym, NNT, that stands for the “number needed to treat” (for one person to benefit).
What “good” looks like
Here’s a screenshot of a review of statin drugs in those with evidence of heart disease:

[click image to enlarge it]
And here’s the same image marked up to show how it is that there is a net gain of life when statins are administered to those with known heart disease:

[click image to enlarge it]
Because more people live when some people take statins, there is “net benefit” to prescribing them for those who have known heart disease. There are two possible harms of interest, diabetes and muscle damage.
Muscle damage can likely be prevented with Coenzyme Q-10, though doctors in the USA don’t co-prescribe it with statins as much as European doctors do.
More worrisome is type 2 diabetes. A national study in Germany revealed that it can make you 82% more likely to die. Even if it is assumed that statins cause diabetes on Day 1 of medication, in a cohort of 4,150 patients followed for 5 years, there would still be less than 3 lives lost to diabetes caused by statins — while 50 lives get saved.
Do COVID jabs look “good” — like statins do?
Everyone agrees that Omicron variant isn’t as lethal as prior variants. The question is over how much less lethal it is, not whether it is less lethal. A South African study put Omicron down as being 78.7% less lethal than “previous variants” there.
The UK Technical Briefing #25, along with another UK report of over 1 million infections, reveals that Omicron is 87% less lethal than pre-Delta COVID variants.
Using assumptions about lethality, spread, and “vaccine effectiveness” — you can estimate the absolute risk reduction (ARR) and, therefore, the number-needed-to-vaccinate (NNV) in order to avert one COVID death.
Because there are 15 reports of death in VAERS for every million COVID jabs given, and because passive surveillance systems very likely capture somewhere from 2% to 18% of background adverse events, you can also estimate the harm from COVID jabs, and relate it to the expected benefit:

[click image to enlarge it]
As you can tell from the estimates, “vaccinating” kids is likely to cause hundreds of child deaths for every child’s life that gets saved by averting a death from Omicron variant COVID.
Even vaccinating 23 year-olds does not have any estimated net benefit, but instead has estimated net harm. These estimates are straight from VAERS along with adjustments based on estimated capture rates of the VAERS system.
But even data from Nordic nations on excess strokes per million vaccine doses, especially with Moderna, along with the death rate from strokes, reveals that 23 year-olds already have negative risk:benefit from just this one single adverse event:
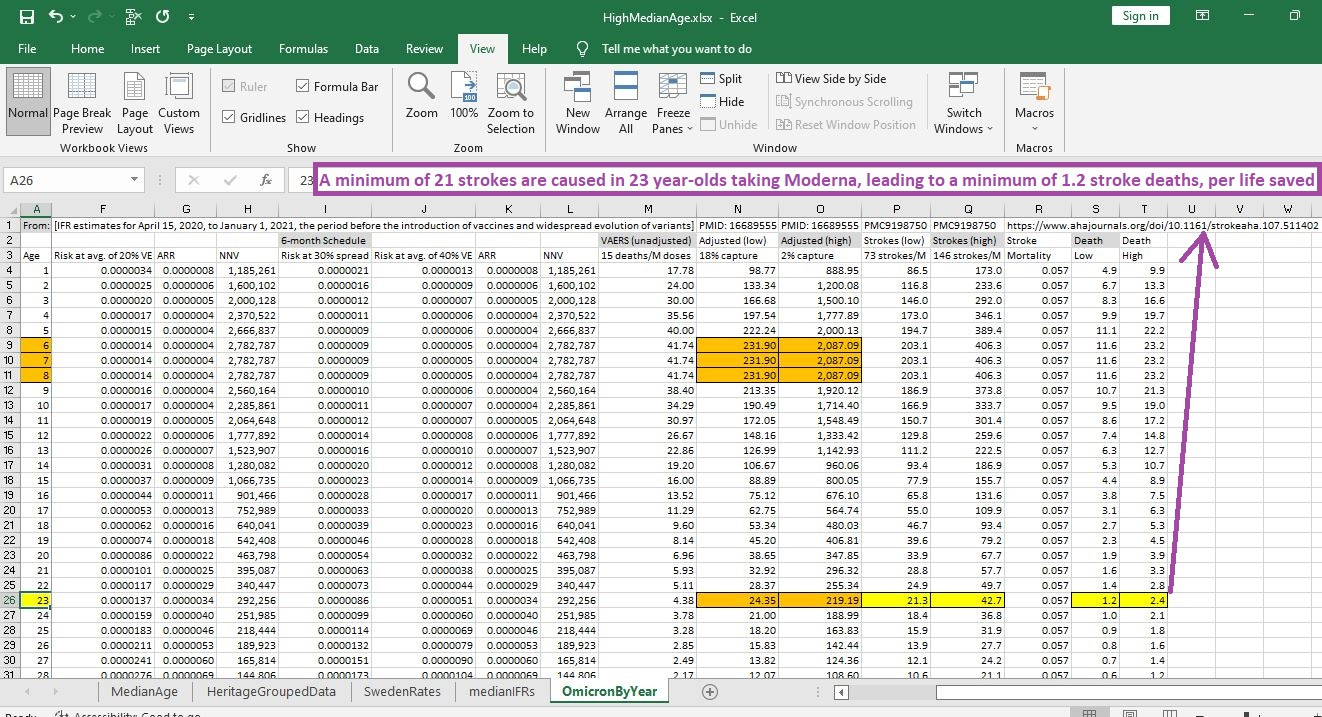
[click image to enlarge it]
When looking for the minimum age when the COVID jabs begin to have a net benefit to them, the estimates reveal that no one under age 50 — with possible exceptions based individualized circumstances — should expect any net benefit from the COVID jab:
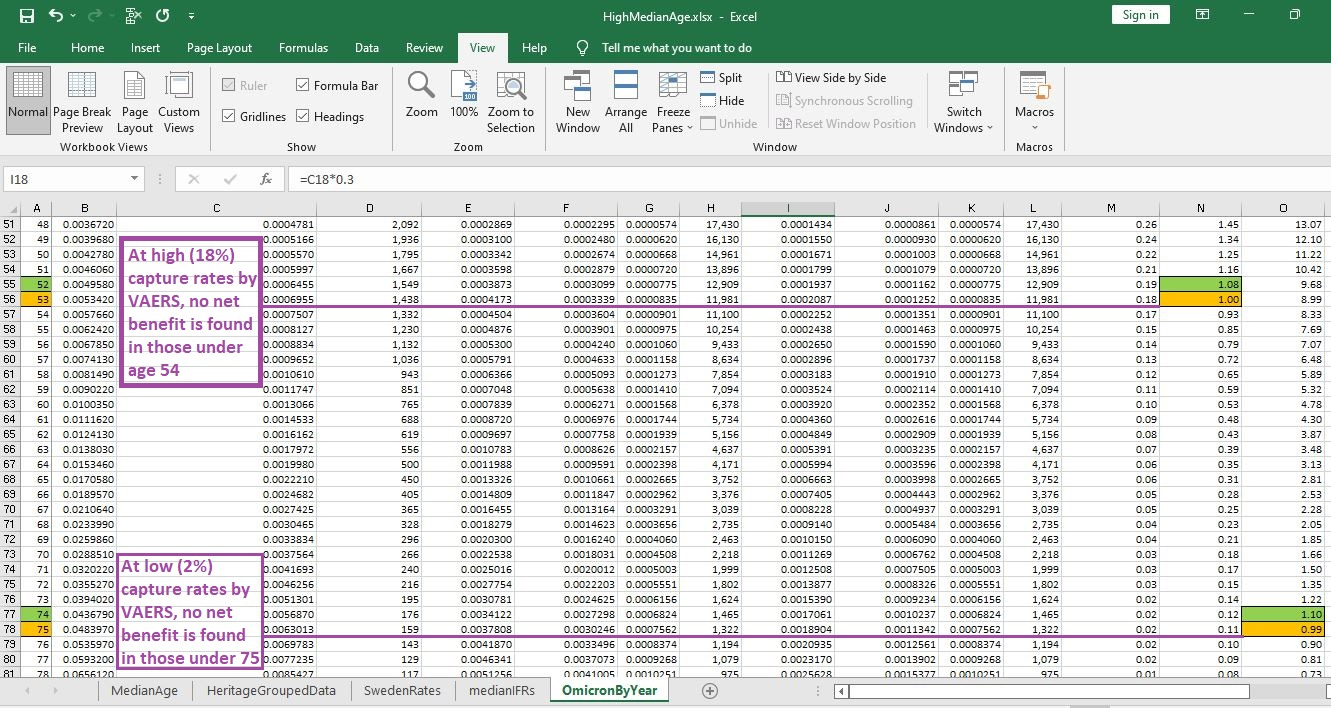
[click image to enlarge it]
Reference
[evidence-based medicine website which shows you what “good” looks like, when objectively evaluating medicines] — TheNNT. https://www.thennt.com/home-nnt/
[type 2 diabetes can make you 82% more likely to die] — All-cause mortality in adults with and without type 2 diabetes: findings from the national health monitoring in Germany. https://drc.bmj.com/content/5/1/e000451
[early COVID IFR by age from age 1 up to age 100] — Variation in the COVID-19 infection–fatality ratio by age, time, and geography during the pre-vaccine era: a systematic analysis. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02867-1/fulltext
[From ~700,000 cases confirmed by sequencing, Delta was 42% as fatal as Alpha] — Table 3. Number of confirmed and probable cases by variant as of 11 October 2021. UK Technical Briefing #25. https://www.gov.uk/government/publications/investigation-of-sars-cov-2-variants-technical-briefings
[From 1.5 million confirmed cases, Omicron is 31% as lethal as Delta, making Omicron much safer than the seasonal flu] — Nyberg T, Ferguson NM, Nash SG, Webster HH, Flaxman S, Andrews N, Hinsley W, Bernal JL, Kall M, Bhatt S, Blomquist P, Zaidi A, Volz E, Aziz NA, Harman K, Funk S, Abbott S; COVID-19 Genomics UK (COG-UK) consortium, Hope R, Charlett A, Chand M, Ghani AC, Seaman SR, Dabrera G, De Angelis D, Presanis AM, Thelwall S. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022 Mar 16:S0140-6736(22)00462-7. doi: 10.1016/S0140-6736(22)00462-7. Epub ahead of print. PMID: 35305296; PMCID: PMC8926413. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8926413/
[an almost 80% reduced lethality of Omicron variant] — Liu Y, Yu Y, Zhao Y, He D. Reduction in the infection fatality rate of Omicron variant compared with previous variants in South Africa. Int J Infect Dis. 2022 Jul;120:146-149. doi: 10.1016/j.ijid.2022.04.029. Epub 2022 Apr 21. PMID: 35462038; PMCID: PMC9022446. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9022446/
[Lancet study showing 4471 reported deaths in VAERS for 298.8 million vaccine doses (15 deaths/M doses)] — Safety of mRNA vaccines administered during the initial 6 months of the US COVID-19 vaccination programme: an observational study of reports to the Vaccine Adverse Event Reporting System and v-safe. Available: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(22)00054-8/fulltext#%20
[The plausible range of adverse event (AE) capture rates goes from a low of 2% up to a high of 18%: the interquartile range of the 37 studies reviewed] — Hazell L, Shakir SA. Under-reporting of adverse drug reactions : a systematic review. Drug Saf. 2006;29(5):385-96. doi: 10.2165/00002018-200629050-00003. PMID: 16689555. https://pubmed.ncbi.nlm.nih.gov/16689555/
[up to 146 excess strokes per million doses (Moderna)] — Dag Berild J, Bergstad Larsen V, Myrup Thiesson E, Lehtonen T, Grøsland M, Helgeland J, Wolhlfahrt J, Vinsløv Hansen J, Palmu AA, Hviid A. Analysis of Thromboembolic and Thrombocytopenic Events After the AZD1222, BNT162b2, and MRNA-1273 COVID-19 Vaccines in 3 Nordic Countries. JAMA Netw Open. 2022 Jun 1;5(6):e2217375. doi: 10.1001/jamanetworkopen.2022.17375. PMID: 35699955; PMCID: PMC9198750. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9198750/
[age-specific risk of death from stroke] — Stroke Outcome in Those Over 80. https://www.ahajournals.org/doi/10.1161/strokeaha.107.511402
[the best average vaccine effectiveness, against serious outcomes such as hospitalization, is 40% VE over a course of 6 months, and 20% VE over 12 months] — Updates on COVID-19 Vaccine Effectiveness during Omicron. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2022-09-01/04-COVID-Link-Gelles-508.pdf

[purple markings added; click image to enlarge]