

Key Term: “RSV” = respiratory syncytial virus
Norman Fenton and Martin Neil recently published a substack post on the monoclonal antibody, Clesrovimab, offered for RSV, and which had survived a review by the ACIP committee, due to shoddy evidence and possible in-house trickery by the sponsors of it. Here, I independently confirm one of their findings regarding the “Merck2” trial:
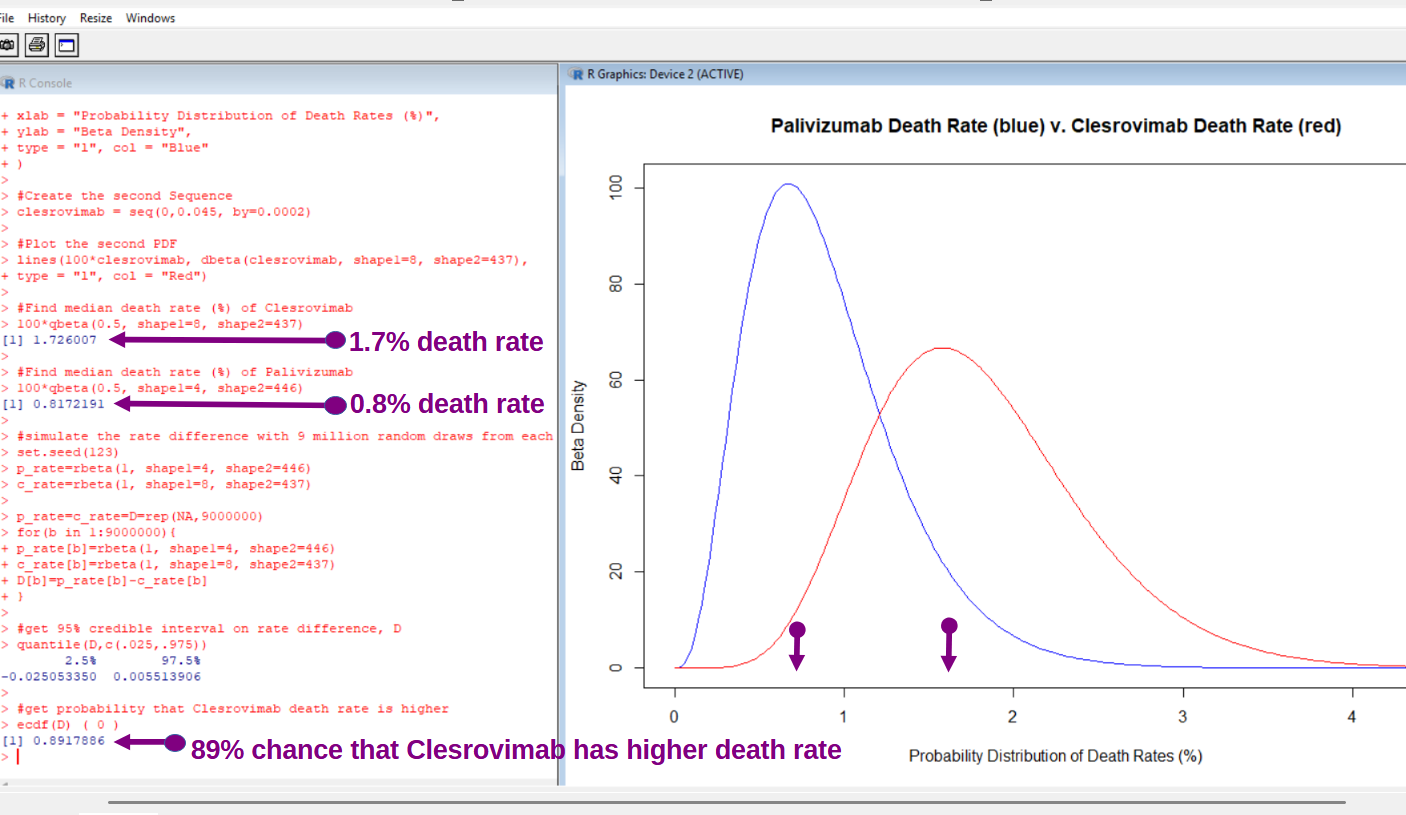
[click to enlarge]
The distribution of possible death rates for each substance shows up at right, and red is the new Clesrovimab product. As shown in the first graphic at Fenton & Neil’s substack, the Merck2 trial was a head-to-head study against the related monoclonal antibody, Palivizumab — having 4 deaths in 450 when Clesrovimab had 8 in 445.
Because the beta distributions narrow as you add more data to them, this analysis is also a Bayesian analysis. To recap, the prime question asked, and answered, by Bayesian analysis is:
Given the data, how likely are various parameter values?
In contrast, the prime question asked and answered with the Frequentist approach is this one:
Given an assumption about the “true rate”, what chance did our sample have to exist?
The “assumption about the true rate” is called the Null Hypothesis and, in the Frequentist approach, the chance of witnessing the data is computed under the assumption that the Null Hypothesis was the underlying truth of the matter. The Bayesian approach gets you the answer you always wanted though:
The probability distribution of all of the possibilities, given the data observed.
Looking at the blue curve, you can visually tell that a death rate of 4% for Palivizumab has “a snowball’s chance in hell” of being true, given the data. And that is the beauty of the analysis, it shows you all of the chances of all possible realities. To verify a claim that Clesrovimab is more deadly is almost 90% likely, 9 million simulations were run.
Drawing randomly from each beta distribution, and then subtracting Clesrovimab’s random death rate from Palivizumab’s, the 9 million rate differences tended negative. Actually, 89% of those 9 million rate differences favored Palivizumab. Because my method is different from that used by Fenton & Neil, it corroborates their finding.
With an almost 90% chance of being more deadly, you would hope that some pause would be given when put under review. But this time, it looks as if the ACIP committee got sold a sketchy bill-of-goods dressed-up with some fancy statistical chicanery which did not allow for the truly-meaningful questions to get answered.
Could you explain that in simple terms for me. I’m not a scientist sadly